Madison T Preib, Maia R Emden, Naomi C Sacks, Fanny S Mitrani-Gold, Shinyoung Ju, Yoshiaki Kawano, Shinya Kawamatsu, Ashish V Joshi
{"title":"Prevalence and economic evaluation of acute uncomplicated cystitis in women from Japan: a retrospective cohort study.","authors":"Madison T Preib, Maia R Emden, Naomi C Sacks, Fanny S Mitrani-Gold, Shinyoung Ju, Yoshiaki Kawano, Shinya Kawamatsu, Ashish V Joshi","doi":"10.1093/jacamr/dlaf178","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although Japanese guidelines recommend fluoroquinolones (FQs) and cephalosporins for AUC (acute uncomplicated cystitis) treatment, the emergence of FQ-resistant uropathogens and inappropriate use of antibiotics may lead to treatment failure (TF), and increased healthcare costs. There is a need to understand the epidemiology, treatment patterns, and healthcare cost implications associated with AUC in Japan.</p><p><strong>Methods: </strong>This retrospective cohort study used the Japanese Medical Database Centre database (1 October 2015-30 November 2021). Female patients (≥18 years) had an AUC diagnosis in the same month as ≥1 oral antibiotic prescription claim in the outpatient setting. The population was stratified into cohorts by TF status and history of AUC recurrence prior to index (pre-index recurrence). Baseline demographics were evaluated in the 12-month pre-index period and age standardized prevalence of AUC was calculated. Treatment patterns and AUC-related costs [2022 Japanese Yen (¥)], were reported for the post-index follow-up period.</p><p><strong>Results: </strong>Of 71 476 total patients, 62.46% were aged <50 years. Patients had evidence of TF (<i>n</i> = 3742; 5.24%) and pre-index recurrence (<i>n</i> = 3206; 4.49%). The age standardized prevalence of AUC (2016-2021) decreased from 8.62% to 6.02%, with up to 3.9 million women affected each year. A high proportion of patients with TF received FQs (45.48%) and third generation cephalosporins (43.37%). The mean total AUC-related costs were ¥14 905 and pharmacy costs were ¥1059 per patient, per index AUC episode.</p><p><strong>Conclusion: </strong>Healthcare providers should consider the cost implications for patients with antibiotic TF or a history of AUC recurrence when selecting antibiotics for empiric treatment in Japan.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"7 5","pages":"dlaf178"},"PeriodicalIF":3.3000,"publicationDate":"2025-10-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12531626/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlaf178","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although Japanese guidelines recommend fluoroquinolones (FQs) and cephalosporins for AUC (acute uncomplicated cystitis) treatment, the emergence of FQ-resistant uropathogens and inappropriate use of antibiotics may lead to treatment failure (TF), and increased healthcare costs. There is a need to understand the epidemiology, treatment patterns, and healthcare cost implications associated with AUC in Japan.
Methods: This retrospective cohort study used the Japanese Medical Database Centre database (1 October 2015-30 November 2021). Female patients (≥18 years) had an AUC diagnosis in the same month as ≥1 oral antibiotic prescription claim in the outpatient setting. The population was stratified into cohorts by TF status and history of AUC recurrence prior to index (pre-index recurrence). Baseline demographics were evaluated in the 12-month pre-index period and age standardized prevalence of AUC was calculated. Treatment patterns and AUC-related costs [2022 Japanese Yen (¥)], were reported for the post-index follow-up period.
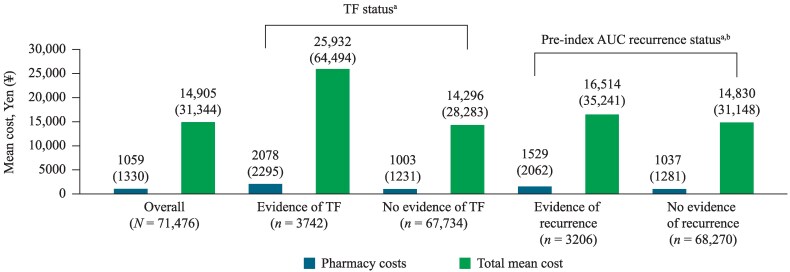
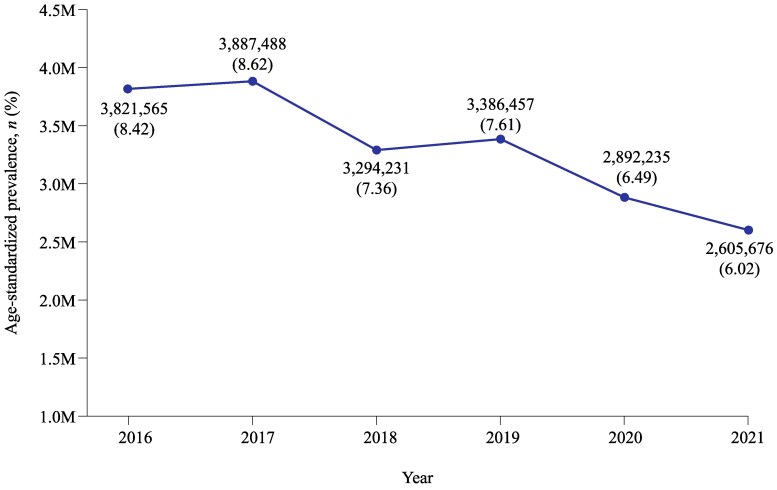
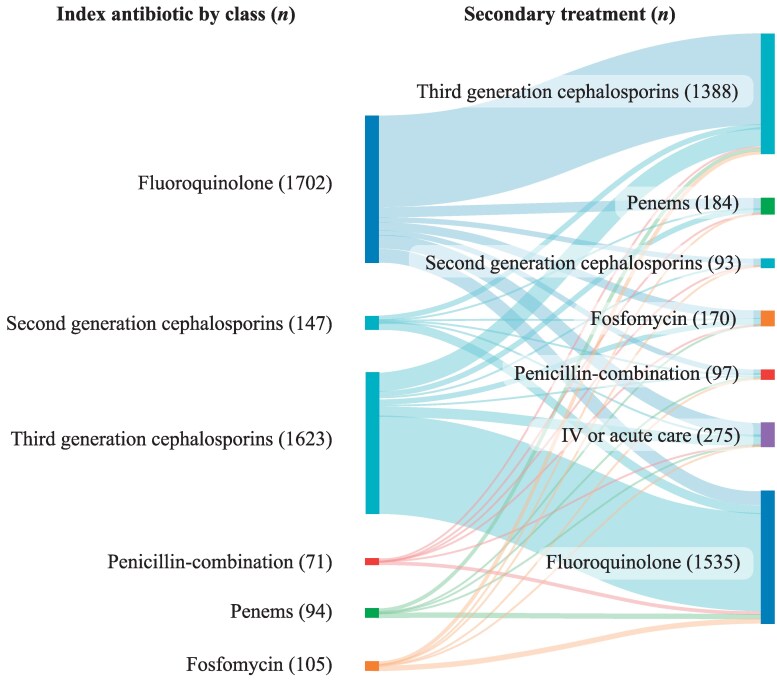
Results: Of 71 476 total patients, 62.46% were aged <50 years. Patients had evidence of TF (n = 3742; 5.24%) and pre-index recurrence (n = 3206; 4.49%). The age standardized prevalence of AUC (2016-2021) decreased from 8.62% to 6.02%, with up to 3.9 million women affected each year. A high proportion of patients with TF received FQs (45.48%) and third generation cephalosporins (43.37%). The mean total AUC-related costs were ¥14 905 and pharmacy costs were ¥1059 per patient, per index AUC episode.
Conclusion: Healthcare providers should consider the cost implications for patients with antibiotic TF or a history of AUC recurrence when selecting antibiotics for empiric treatment in Japan.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


