{"title":"Propofol TIVA vs. inhalational anesthesia for spine surgery: in‑hospital mortality and postoperative complications in a nationwide Korean cohort.","authors":"Tak Kyu Oh, Saeyeon Kim, In-Ae Song","doi":"10.1186/s12871-025-03385-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Given propofol's antioxidant and anti‑inflammatory properties compared with volatile/inhalational agents, we aimed to evaluate the association between anesthetic technique and both in‑hospital mortality and postoperative complications following spinal surgery.</p><p><strong>Methods: </strong>In this retrospective, population‑based cohort study, we used South Korea's National Health Insurance Service database to identify adult patients (≥ 18 years) who underwent spinal surgery between January 1, 2016 and December 31, 2021. Primary outcomes were in‑hospital mortality and postoperative complications. Propensity score (PS) matching (1:1) was employed to balance baseline characteristics between the total intravenous anesthesia (TIVA) and volatile/inhalational anesthesia (INH) groups.</p><p><strong>Results: </strong>Among 708,387 patients, 264,728 (37.4%) received TIVA and 443,659 (62.6%) received INH. After PS matching, 460,654 patients remained (230,327 per group). In the PS‑matched cohort, TIVA was associated with significantly lower odds of in‑hospital mortality (OR 0.85; 95% CI 0.80-0.89; P = 0.004) and postoperative complications (11.8% vs. 14.2%; OR 0.81; 95% CI 0.80-0.82; P < 0.001) compared with INH. In the full cohort, multivariable logistic regression confirmed these findings: TIVA remained linked to reduced in‑hospital mortality (OR 0.74; 95% CI 0.63-0.87; P < 0.001) and fewer postoperative complications (OR 0.71; 95% CI 0.70-0.73; P < 0.001).</p><p><strong>Conclusions: </strong>In this nationwide cohort, propofol‑based TIVA was associated with lower in‑hospital mortality and fewer postoperative complications than volatile/inhalational anesthesia in adult spinal surgery patients. Prospective trials are warranted to confirm these findings.</p><p><strong>Trial registration: </strong>Not applicable.</p>","PeriodicalId":9190,"journal":{"name":"BMC Anesthesiology","volume":"25 1","pages":"508"},"PeriodicalIF":2.6000,"publicationDate":"2025-10-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12533432/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12871-025-03385-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Given propofol's antioxidant and anti‑inflammatory properties compared with volatile/inhalational agents, we aimed to evaluate the association between anesthetic technique and both in‑hospital mortality and postoperative complications following spinal surgery.
Methods: In this retrospective, population‑based cohort study, we used South Korea's National Health Insurance Service database to identify adult patients (≥ 18 years) who underwent spinal surgery between January 1, 2016 and December 31, 2021. Primary outcomes were in‑hospital mortality and postoperative complications. Propensity score (PS) matching (1:1) was employed to balance baseline characteristics between the total intravenous anesthesia (TIVA) and volatile/inhalational anesthesia (INH) groups.
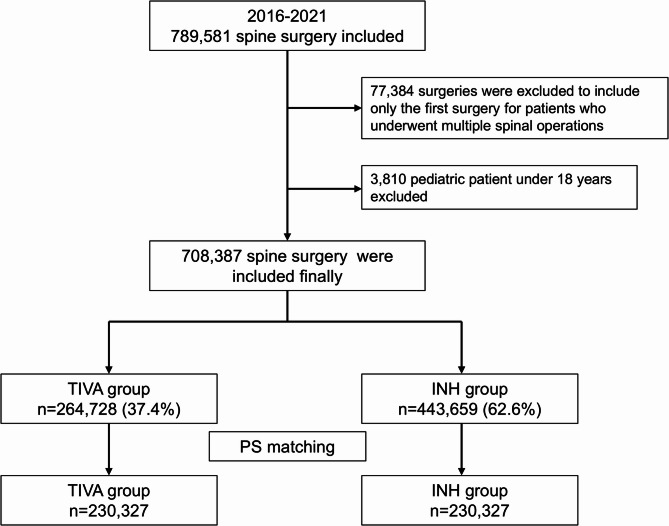
Results: Among 708,387 patients, 264,728 (37.4%) received TIVA and 443,659 (62.6%) received INH. After PS matching, 460,654 patients remained (230,327 per group). In the PS‑matched cohort, TIVA was associated with significantly lower odds of in‑hospital mortality (OR 0.85; 95% CI 0.80-0.89; P = 0.004) and postoperative complications (11.8% vs. 14.2%; OR 0.81; 95% CI 0.80-0.82; P < 0.001) compared with INH. In the full cohort, multivariable logistic regression confirmed these findings: TIVA remained linked to reduced in‑hospital mortality (OR 0.74; 95% CI 0.63-0.87; P < 0.001) and fewer postoperative complications (OR 0.71; 95% CI 0.70-0.73; P < 0.001).
Conclusions: In this nationwide cohort, propofol‑based TIVA was associated with lower in‑hospital mortality and fewer postoperative complications than volatile/inhalational anesthesia in adult spinal surgery patients. Prospective trials are warranted to confirm these findings.
背景:与挥发性/吸入性药物相比,异丙酚具有抗氧化和抗炎特性,我们旨在评估麻醉技术与脊柱手术后住院死亡率和术后并发症之间的关系。方法:在这项基于人群的回顾性队列研究中,我们使用韩国国民健康保险服务数据库来识别2016年1月1日至2021年12月31日期间接受脊柱手术的成年患者(≥18岁)。主要结局是院内死亡率和术后并发症。采用倾向评分(PS)匹配(1:1)来平衡全静脉麻醉(TIVA)组和挥发性/吸入麻醉(INH)组之间的基线特征。结果:708387例患者中,264728例(37.4%)接受了TIVA, 443659例(62.6%)接受了INH。PS匹配后,剩余460,654例患者(每组230,327例)。在PS匹配的队列中,TIVA与院内死亡率(OR 0.85; 95% CI 0.80-0.89; P = 0.004)和术后并发症(11.8% vs. 14.2%; OR 0.81; 95% CI 0.80-0.82; P)相关,结论:在这个全国性队列中,与挥发性/吸入麻醉相比,成人脊柱手术患者基于异丙酚的TIVA与更低的院内死亡率和更少的术后并发症相关。有必要进行前瞻性试验来证实这些发现。试验注册:不适用。
期刊介绍:
BMC Anesthesiology is an open access, peer-reviewed journal that considers articles on all aspects of anesthesiology, critical care, perioperative care and pain management, including clinical and experimental research into anesthetic mechanisms, administration and efficacy, technology and monitoring, and associated economic issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


