Barriers to physical activity and patient profiling in the lifelong maintenance phase of coronary artery disease: a territorial mixed-methods pilot study.
{"title":"Barriers to physical activity and patient profiling in the lifelong maintenance phase of coronary artery disease: a territorial mixed-methods pilot study.","authors":"Morgane Molina, Fabienne Durand, Henri Meric","doi":"10.3389/fresc.2025.1659925","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Despite proven benefits, adherence to physical activity (PA) during the lifelong maintenance phase of cardiac rehabilitation (CR) remains suboptimal. Understanding territorial-specific barriers is essential for developing targeted interventions. This pilot study aimed to (1) identify principal barriers to PA among coronary artery disease (CAD) patients in lifelong maintenance Phase CR in a specific territory of southern France, and (2) characterize distinct patient profiles using unsupervised machine learning.</p><p><strong>Methods: </strong>Socio-demographic data, completion of a full Phase II CR and behavioral characteristics related to PA during the lifelong maintenance Phase were collected with a LimeSurvey questionnaire. A modified Delphi method was employed with CAD patients (<i>n</i> = 26, subsequently, <i>n</i> = 13 in round 2) who had completed a supervised Phase II CR. Barriers were categorized and ranked using Likert scales. K-means clustering analysis was then applied to identify homogeneous patient subgroups based on barrier patterns.</p><p><strong>Results: </strong>Nine barrier categories emerged, with environment (8.3 ± 1.0), motivation (7.7 ± 1.4), and exercise tolerance (6.3 ± 1.2) ranking highest. Kendall's W = 0.64 (<i>p</i> < 0.001) indicated a significant consensus. Three cluster were identified: Cluster 1 (38.46%) characterized by physical deconditioning; Cluster 2 (23.07%) by environmental and motivational constraints; Cluster 3 (38.46%) by organizational limitations. Significant between-cluster differences were observed for: environmental barriers (H = 7.82, <i>p</i> = 0.02), motivation (H = 8.14, <i>p</i> = 0.017), and professional obligations (H = 6.93, <i>p</i> = 0.031).</p><p><strong>Conclusion: </strong>This mixed-methods approach revealed complex, interrelated barriers to PA maintenance. The identification of distinct CAD patient profiles suggests that personalized intervention strategies, rather than one-size-fits-all approaches, may enhance long-term adherence to PA in lifelong maintenance Phase CR.</p>","PeriodicalId":73102,"journal":{"name":"Frontiers in rehabilitation sciences","volume":"6 ","pages":"1659925"},"PeriodicalIF":1.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12521154/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in rehabilitation sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fresc.2025.1659925","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Despite proven benefits, adherence to physical activity (PA) during the lifelong maintenance phase of cardiac rehabilitation (CR) remains suboptimal. Understanding territorial-specific barriers is essential for developing targeted interventions. This pilot study aimed to (1) identify principal barriers to PA among coronary artery disease (CAD) patients in lifelong maintenance Phase CR in a specific territory of southern France, and (2) characterize distinct patient profiles using unsupervised machine learning.
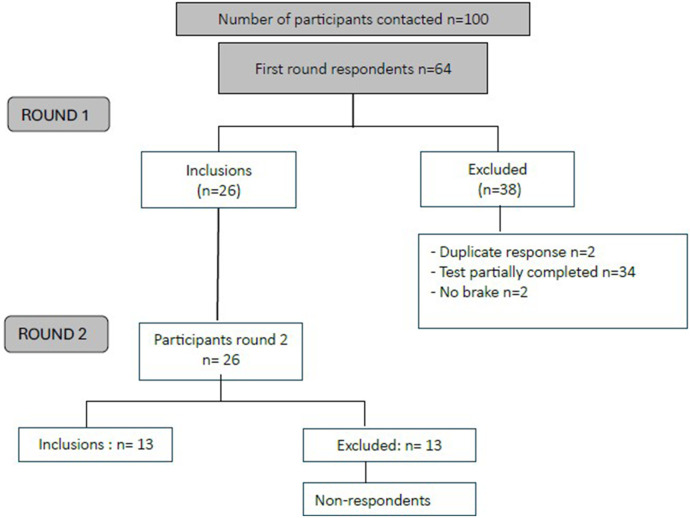
Methods: Socio-demographic data, completion of a full Phase II CR and behavioral characteristics related to PA during the lifelong maintenance Phase were collected with a LimeSurvey questionnaire. A modified Delphi method was employed with CAD patients (n = 26, subsequently, n = 13 in round 2) who had completed a supervised Phase II CR. Barriers were categorized and ranked using Likert scales. K-means clustering analysis was then applied to identify homogeneous patient subgroups based on barrier patterns.
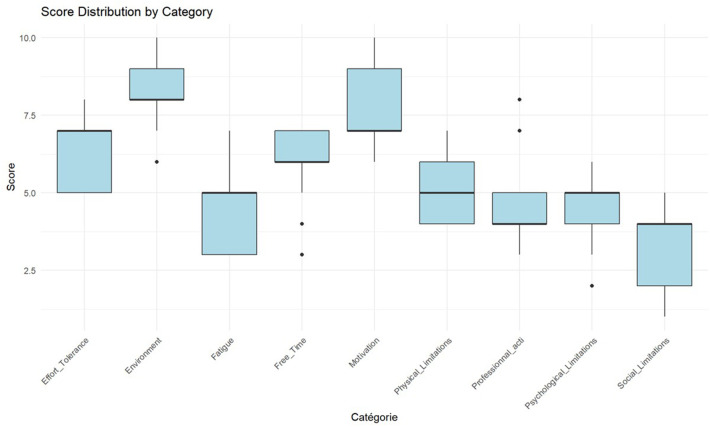
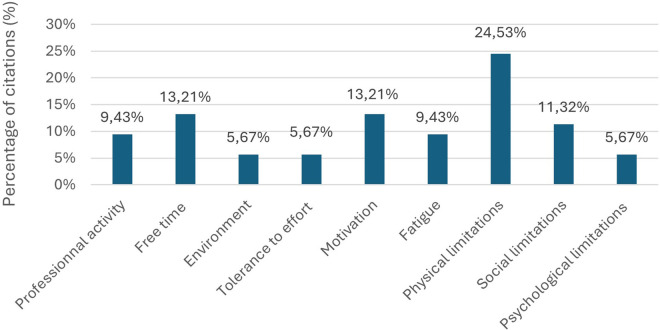
Results: Nine barrier categories emerged, with environment (8.3 ± 1.0), motivation (7.7 ± 1.4), and exercise tolerance (6.3 ± 1.2) ranking highest. Kendall's W = 0.64 (p < 0.001) indicated a significant consensus. Three cluster were identified: Cluster 1 (38.46%) characterized by physical deconditioning; Cluster 2 (23.07%) by environmental and motivational constraints; Cluster 3 (38.46%) by organizational limitations. Significant between-cluster differences were observed for: environmental barriers (H = 7.82, p = 0.02), motivation (H = 8.14, p = 0.017), and professional obligations (H = 6.93, p = 0.031).
Conclusion: This mixed-methods approach revealed complex, interrelated barriers to PA maintenance. The identification of distinct CAD patient profiles suggests that personalized intervention strategies, rather than one-size-fits-all approaches, may enhance long-term adherence to PA in lifelong maintenance Phase CR.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


