Association between early administration of mucoactive agents and in-hospital mortality in patients with pneumonia requiring mechanical ventilation: a nationwide cohort study.
{"title":"Association between early administration of mucoactive agents and in-hospital mortality in patients with pneumonia requiring mechanical ventilation: a nationwide cohort study.","authors":"Akira Sasaki, Mikio Nakajima, Tomohiro Shinozaki, Yusuke Sasabuchi, Hiroyuki Ohbe, Richard H Kaszynski, Yuya Kimura, Kojiro Morita, Tadahiro Goto, Yuki Aiyama, Izumi Nakayama, Hiroki Matsui, Kiyohide Fushimi, Hidenobu Ochiai, Hideo Yasunaga","doi":"10.1186/s40560-025-00826-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with pneumonia requiring mechanical ventilation, increased airway secretions are associated with prolonged mechanical ventilation, but the effect of mucoactive agents remains unclear. The present study aimed to investigate the association between early administration of mucoactive agents and in-hospital mortality in patients with pneumonia requiring mechanical ventilation.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study using the Japanese Diagnosis Procedure Combination database, a nationwide inpatient database. Adult patients were eligible if they had a primary diagnosis of pneumonia and required invasive mechanical ventilation within 2 days of admission, with ventilation continued for ≥ 2 days between April 2012 and March 2023. Patients were divided into those who received at least one mucoactive agent within 2 days after the initiation of mechanical ventilation (mucoactive agent group) and those who did not (control group). Mucoactive agents included ambroxol (oral), bromhexine (oral, intravenous and nebulized), fudosteine (oral), carbocisteine (oral) and N-acetylcysteine (nebulized). We performed a propensity score overlap weighting analysis to compare in-hospital mortality. The number of ventilator-free days at 28 days was assessed as a secondary outcome. We also performed sensitivity analyses using inverse probability of treatment weighting, generalized estimating equations, and doubly robust methods.</p><p><strong>Results: </strong>Eligible patients (n = 10,942) were categorized into the mucoactive agent group (n = 2246) or control group (n = 8696). The most commonly prescribed mucoactive agent was carbocisteine (oral). After overlap weighting, in-hospital mortality was significantly lower in the mucoactive agent group than in the control group (25.2% vs. 27.5%; risk difference, - 2.3%; 95% confidence interval, - 4.4% to - 0.3%; p = 0.028). Ventilator-free days at 28 days did not significantly differ between the mucoactive agent group and the control group. Sensitivity analyses yielded similar results.</p><p><strong>Conclusions: </strong>In patients with ventilated pneumonia, early administration of mucoactive agents was associated with lower in-hospital mortality.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"13 1","pages":"57"},"PeriodicalIF":4.7000,"publicationDate":"2025-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12532859/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-025-00826-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In patients with pneumonia requiring mechanical ventilation, increased airway secretions are associated with prolonged mechanical ventilation, but the effect of mucoactive agents remains unclear. The present study aimed to investigate the association between early administration of mucoactive agents and in-hospital mortality in patients with pneumonia requiring mechanical ventilation.
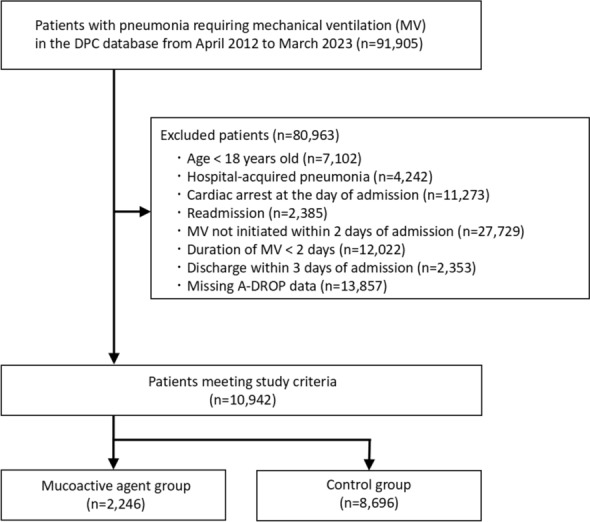
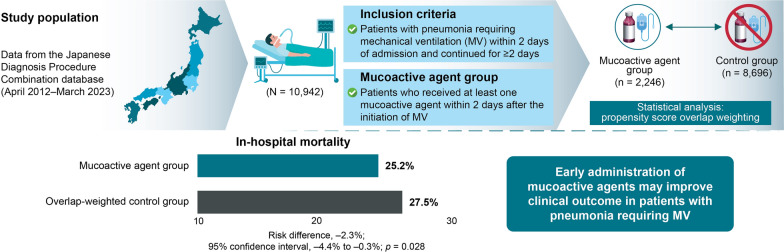
Methods: We conducted a retrospective cohort study using the Japanese Diagnosis Procedure Combination database, a nationwide inpatient database. Adult patients were eligible if they had a primary diagnosis of pneumonia and required invasive mechanical ventilation within 2 days of admission, with ventilation continued for ≥ 2 days between April 2012 and March 2023. Patients were divided into those who received at least one mucoactive agent within 2 days after the initiation of mechanical ventilation (mucoactive agent group) and those who did not (control group). Mucoactive agents included ambroxol (oral), bromhexine (oral, intravenous and nebulized), fudosteine (oral), carbocisteine (oral) and N-acetylcysteine (nebulized). We performed a propensity score overlap weighting analysis to compare in-hospital mortality. The number of ventilator-free days at 28 days was assessed as a secondary outcome. We also performed sensitivity analyses using inverse probability of treatment weighting, generalized estimating equations, and doubly robust methods.
Results: Eligible patients (n = 10,942) were categorized into the mucoactive agent group (n = 2246) or control group (n = 8696). The most commonly prescribed mucoactive agent was carbocisteine (oral). After overlap weighting, in-hospital mortality was significantly lower in the mucoactive agent group than in the control group (25.2% vs. 27.5%; risk difference, - 2.3%; 95% confidence interval, - 4.4% to - 0.3%; p = 0.028). Ventilator-free days at 28 days did not significantly differ between the mucoactive agent group and the control group. Sensitivity analyses yielded similar results.
Conclusions: In patients with ventilated pneumonia, early administration of mucoactive agents was associated with lower in-hospital mortality.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


