{"title":"Where does the fluid go?","authors":"Robert G Hahn","doi":"10.1186/s13613-025-01579-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Liberal administration of crystalloid fluid is often required to maintain adequate tissue perfusion when treating life-threatening conditions. Current knowledge indicates that either overhydration or underhydration can promote complications. This review describes how fluid distributes between body compartments, with the aim of finding insights into pathophysiological mechanisms that can explain why fluid overload may cause complications and even be fatal.</p><p><strong>Main text: </strong>The skin, intestinal wall, and lungs are known primary locations of excess amounts of crystalloid fluid in humans. Microscopic studies in animals show that infusion of > 100 mL/kg of crystalloid fluid also causes interstitial dilatation and swelling of the heart, tissue breakup, and cardiac hypoxia. Volume kinetic analysis has identified several factors that promote peripheral edema during general anesthesia. Volume kinetics also shows that increasing volumes of crystalloid fluid sequentially expands three body fluid compartments: the plasma, a fast-exchange interstitial volume, and a more remote slow-exchange interstitial volume (in scientific jargon called \"the third fluid space\"). In settings of overhydration, the slow-exchange space operates as an overflow reservoir and quickly begins to accumulate fluid when the fast-exchange compartment has increased by 600-800 mL, which corresponds to infusing approximately 1.3-1.5 L of crystalloid fluid into the plasma over 30 min. Apart from overhydration, accumulation of fluid in the slow-exchange space occurs in inflammatory conditions, whereby cytokines and vasoactive molecules create a suction pressure that withdraws fluid from the fast-exchange space. This suction decreases lymphatic flow, causing hypovolemia and hypoalbuminemia in addition to peripheral edema. Preeclampsia and sepsis are examples of this complex kinetic situation. Albumin (20%), a hyper-oncotic colloid, might be used to modify peripheral edema by recruiting interstitial (lymphatic) fluid and stimulating diuresis.</p><p><strong>Conclusion: </strong>Excess amounts of crystalloid fluid accumulate in body regions, such as the skin and intestinal walls, that have a high compliance for volume expansion. The heart is potentially a key trouble spot in severe overhydration. Accumulation of fluid in an interstitial fluid space that equilibrates slowly with the plasma volume occurs in settings of overhydration and inflammation. Pathophysiological mechanisms that explain the complications and fatal outcomes of overhydration are insufficiently known in humans.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"156"},"PeriodicalIF":5.5000,"publicationDate":"2025-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12521718/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01579-0","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Liberal administration of crystalloid fluid is often required to maintain adequate tissue perfusion when treating life-threatening conditions. Current knowledge indicates that either overhydration or underhydration can promote complications. This review describes how fluid distributes between body compartments, with the aim of finding insights into pathophysiological mechanisms that can explain why fluid overload may cause complications and even be fatal.
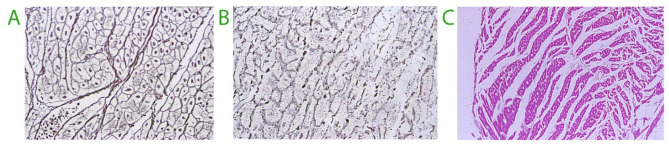
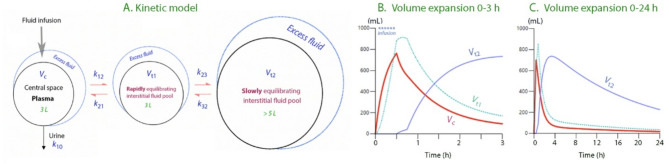
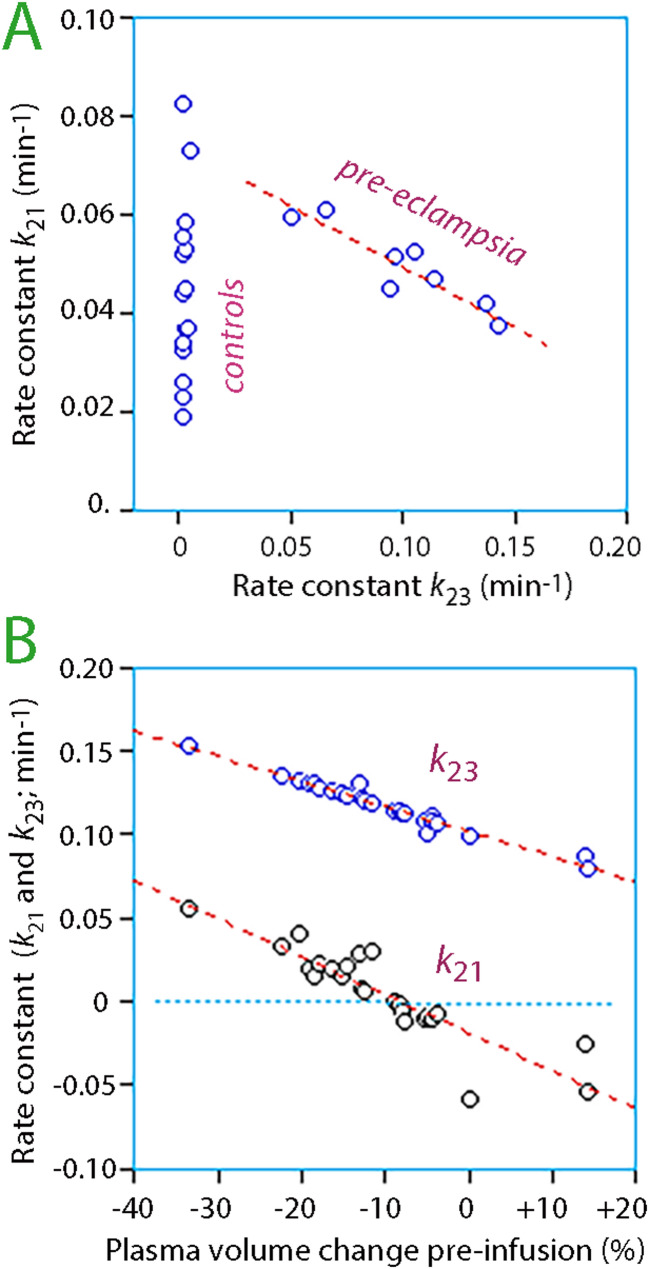
Main text: The skin, intestinal wall, and lungs are known primary locations of excess amounts of crystalloid fluid in humans. Microscopic studies in animals show that infusion of > 100 mL/kg of crystalloid fluid also causes interstitial dilatation and swelling of the heart, tissue breakup, and cardiac hypoxia. Volume kinetic analysis has identified several factors that promote peripheral edema during general anesthesia. Volume kinetics also shows that increasing volumes of crystalloid fluid sequentially expands three body fluid compartments: the plasma, a fast-exchange interstitial volume, and a more remote slow-exchange interstitial volume (in scientific jargon called "the third fluid space"). In settings of overhydration, the slow-exchange space operates as an overflow reservoir and quickly begins to accumulate fluid when the fast-exchange compartment has increased by 600-800 mL, which corresponds to infusing approximately 1.3-1.5 L of crystalloid fluid into the plasma over 30 min. Apart from overhydration, accumulation of fluid in the slow-exchange space occurs in inflammatory conditions, whereby cytokines and vasoactive molecules create a suction pressure that withdraws fluid from the fast-exchange space. This suction decreases lymphatic flow, causing hypovolemia and hypoalbuminemia in addition to peripheral edema. Preeclampsia and sepsis are examples of this complex kinetic situation. Albumin (20%), a hyper-oncotic colloid, might be used to modify peripheral edema by recruiting interstitial (lymphatic) fluid and stimulating diuresis.
Conclusion: Excess amounts of crystalloid fluid accumulate in body regions, such as the skin and intestinal walls, that have a high compliance for volume expansion. The heart is potentially a key trouble spot in severe overhydration. Accumulation of fluid in an interstitial fluid space that equilibrates slowly with the plasma volume occurs in settings of overhydration and inflammation. Pathophysiological mechanisms that explain the complications and fatal outcomes of overhydration are insufficiently known in humans.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


