Retrospective Evaluation and Analysis of Pharmacoequity with Guideline-directed Medical Therapy in Heart Failure with Reduced Ejection Fraction (REAP-HF).
Morgan Streett, Anna Jacobs, Jennifer Twilla, Kaulin Duncan, Geeth Nadella, Drew A Wells
{"title":"Retrospective Evaluation and Analysis of Pharmacoequity with Guideline-directed Medical Therapy in Heart Failure with Reduced Ejection Fraction (REAP-HF).","authors":"Morgan Streett, Anna Jacobs, Jennifer Twilla, Kaulin Duncan, Geeth Nadella, Drew A Wells","doi":"10.24926/iip.v16i1.6626","DOIUrl":null,"url":null,"abstract":"<p><p><i>Introduction:</i> Patients with heart failure with reduced ejection fraction (HFrEF) who are optimized on guideline-directed medical therapy (GDMT) have improved outcomes; however, medication access and affordability are potential barriers to achieving pharmacoequity. This study sought to compare rates of HFrEF GDMT prescribing at hospital discharge across prescription insurance status groups. <i>Methods:</i> This was a single-center, retrospective cohort study of adult HFrEF patients. Patients were grouped according to prescription insurance status. The primary outcome was the percentage of HFrEF patients prescribed quadruple GDMT at hospital discharge. Key secondary outcomes included the presence of contraindications to therapy and 30-day all-cause readmission rates. The study was approved by the Institutional Review Board at the University of Tennessee Health Science Center. <i>Results:</i> Among the 200 included patients, 63% were male and 92% were black. Discharge on quadruple GDMT across insurance groups was 18% for Medicare Part D, 24% for Medicaid, 24% for commercial, and 33% for uninsured. There was no difference between insurance groups in rates of prescribed quadruple GDMT at hospital discharge (p=0.302) or 30-day hospital readmission (p=0.665). Additionally, there was a significant increase in the number of uninsured patients on quadruple GDMT after hospitalization compared to pre-hospitalization (13% vs 33%, p=0.002). Eighty percent of all patients had a contraindication to at least one GDMT agent. <i>Conclusion:</i> There was no difference in rates of prescribed quadruple GDMT at hospital discharge based on insurance status. However, this study did elucidate the impact of medication access programs improving pharmacoequity in the uninsured patient population.</p>","PeriodicalId":501014,"journal":{"name":"Innovations in pharmacy","volume":"16 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12509711/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovations in pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24926/iip.v16i1.6626","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
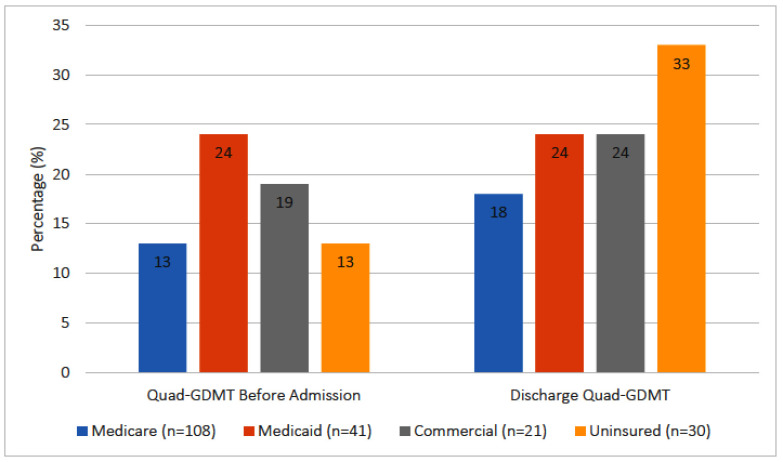
Introduction: Patients with heart failure with reduced ejection fraction (HFrEF) who are optimized on guideline-directed medical therapy (GDMT) have improved outcomes; however, medication access and affordability are potential barriers to achieving pharmacoequity. This study sought to compare rates of HFrEF GDMT prescribing at hospital discharge across prescription insurance status groups. Methods: This was a single-center, retrospective cohort study of adult HFrEF patients. Patients were grouped according to prescription insurance status. The primary outcome was the percentage of HFrEF patients prescribed quadruple GDMT at hospital discharge. Key secondary outcomes included the presence of contraindications to therapy and 30-day all-cause readmission rates. The study was approved by the Institutional Review Board at the University of Tennessee Health Science Center. Results: Among the 200 included patients, 63% were male and 92% were black. Discharge on quadruple GDMT across insurance groups was 18% for Medicare Part D, 24% for Medicaid, 24% for commercial, and 33% for uninsured. There was no difference between insurance groups in rates of prescribed quadruple GDMT at hospital discharge (p=0.302) or 30-day hospital readmission (p=0.665). Additionally, there was a significant increase in the number of uninsured patients on quadruple GDMT after hospitalization compared to pre-hospitalization (13% vs 33%, p=0.002). Eighty percent of all patients had a contraindication to at least one GDMT agent. Conclusion: There was no difference in rates of prescribed quadruple GDMT at hospital discharge based on insurance status. However, this study did elucidate the impact of medication access programs improving pharmacoequity in the uninsured patient population.
导论:心力衰竭伴射血分数降低(HFrEF)的患者在指南导向的药物治疗(GDMT)上进行了优化,改善了预后;然而,药物可及性和可负担性是实现药物公平的潜在障碍。本研究旨在比较不同处方保险状态组出院时HFrEF GDMT处方的比率。方法:这是一项针对成人HFrEF患者的单中心、回顾性队列研究。根据处方保险状况对患者进行分组。主要结局是HFrEF患者出院时服用四倍GDMT的百分比。主要次要结局包括治疗禁忌症的存在和30天全因再入院率。这项研究得到了田纳西大学健康科学中心机构审查委员会的批准。结果:纳入的200例患者中,男性占63%,黑人占92%。医疗保险D部分为18%,医疗补助为24%,商业保险为24%,无保险为33%。两保险组在出院时规定的四倍GDMT比率(p=0.302)或30天再入院率(p=0.665)没有差异。此外,与住院前相比,住院后四倍GDMT的未参保患者数量显著增加(13% vs 33%, p=0.002)。80%的患者至少有一种GDMT药物的禁忌症。结论:不同保险状况患者出院时四重GDMT处方率无差异。然而,本研究确实阐明了药物获取计划对改善无保险患者群体药物公平的影响。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


