{"title":"Early Prophylactic Anticoagulation and In-Hospital Mortality in Patients with Severe Acute Pancreatitis: A Retrospective Cohort Study.","authors":"Haodong Zhao, Hui Liu, Jiongjiong Cheng, Jia Chen, Shuo Li, Yaowei Sun, Yu Wang","doi":"10.2147/OAEM.S539104","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To investigate the association between early prophylactic anticoagulation and in-hospital mortality in ICU patients with severe acute pancreatitis.</p><p><strong>Patients and methods: </strong>This retrospective cohort study used data from the MIMIC-IV database (v3.1), including adult ICU patients diagnosed with SAP between 2008 and 2019. Patients receiving therapeutic anticoagulation were excluded. Early prophylactic anticoagulation was defined as subcutaneous heparin or enoxaparin administered within 24 hours of ICU admission. The primary outcome was in-hospital mortality. Multivariable Cox regression models with multiple imputation and propensity score matching were used to adjust for confounding.</p><p><strong>Results: </strong>Among 1341 eligible patients, 286 (21.3%) received early prophylactic anticoagulation. While crude in-hospital mortality was not significantly different between groups, patients receiving early anticoagulation had significantly lower in-hospital mortality (Log-rank P = 0.015). Multivariable Cox models confirmed a consistent protective association across imputed datasets (HRs ranging from 0.60 to 0.62; all P < 0.05). Subgroup analysis showed no significant interaction across age, gender, or comorbidity status. After 1:1 propensity score matching (n = 284 pairs), the mortality benefit persisted (HR = 0.51; 95% CI: 0.32-0.82; P = 0.005). Additional sensitivity analyses yielded similar results.</p><p><strong>Conclusion: </strong>Early prophylactic anticoagulation within 24 hours of ICU admission was associated with reduced in-hospital mortality in patients with severe acute pancreatitis. These findings suggest potential benefits of early anticoagulation in this high-risk population and warrant further prospective validation.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"17 ","pages":"289-300"},"PeriodicalIF":1.5000,"publicationDate":"2025-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12506791/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S539104","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To investigate the association between early prophylactic anticoagulation and in-hospital mortality in ICU patients with severe acute pancreatitis.
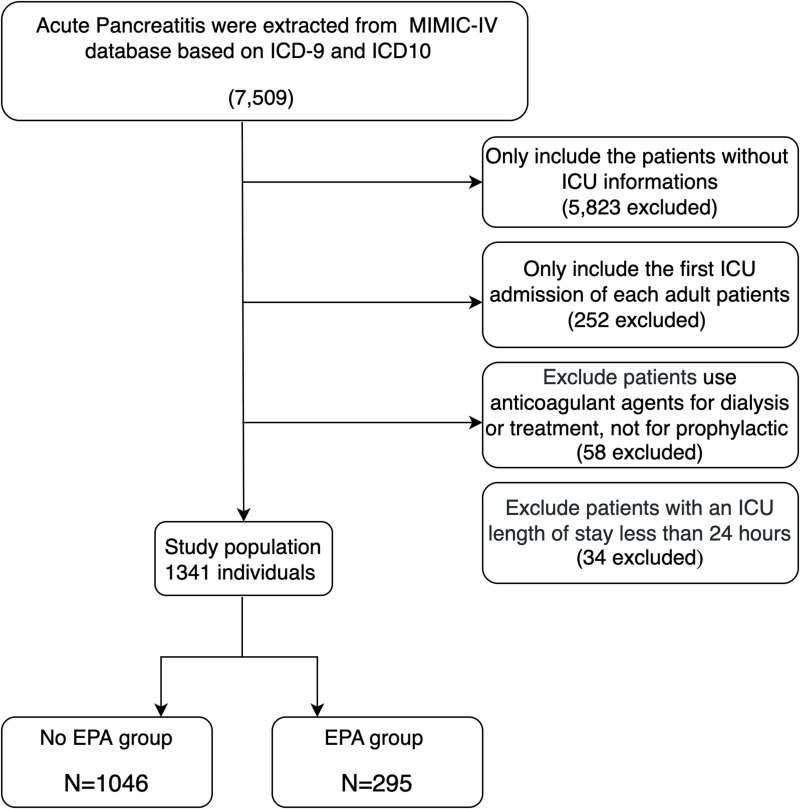
Patients and methods: This retrospective cohort study used data from the MIMIC-IV database (v3.1), including adult ICU patients diagnosed with SAP between 2008 and 2019. Patients receiving therapeutic anticoagulation were excluded. Early prophylactic anticoagulation was defined as subcutaneous heparin or enoxaparin administered within 24 hours of ICU admission. The primary outcome was in-hospital mortality. Multivariable Cox regression models with multiple imputation and propensity score matching were used to adjust for confounding.
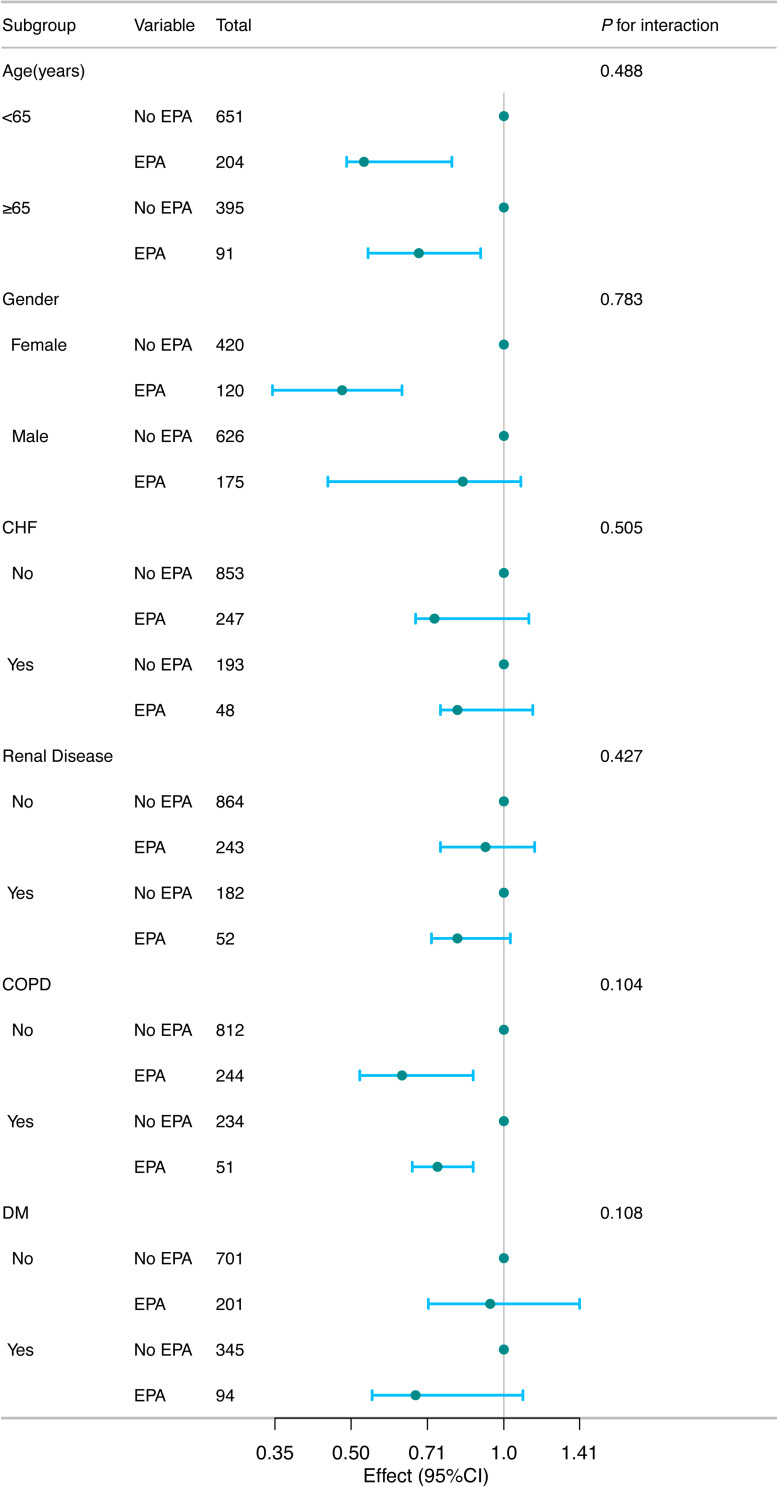
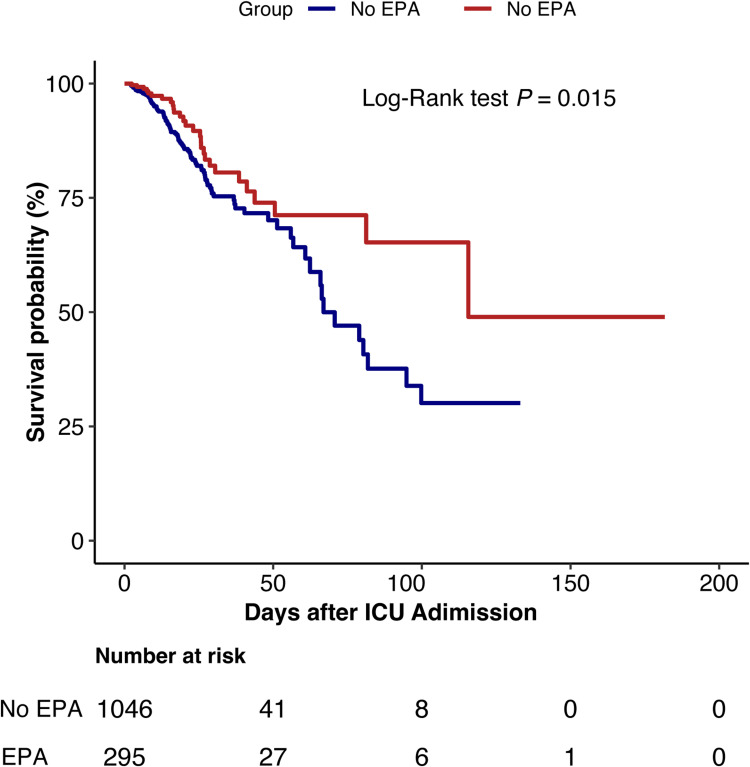
Results: Among 1341 eligible patients, 286 (21.3%) received early prophylactic anticoagulation. While crude in-hospital mortality was not significantly different between groups, patients receiving early anticoagulation had significantly lower in-hospital mortality (Log-rank P = 0.015). Multivariable Cox models confirmed a consistent protective association across imputed datasets (HRs ranging from 0.60 to 0.62; all P < 0.05). Subgroup analysis showed no significant interaction across age, gender, or comorbidity status. After 1:1 propensity score matching (n = 284 pairs), the mortality benefit persisted (HR = 0.51; 95% CI: 0.32-0.82; P = 0.005). Additional sensitivity analyses yielded similar results.
Conclusion: Early prophylactic anticoagulation within 24 hours of ICU admission was associated with reduced in-hospital mortality in patients with severe acute pancreatitis. These findings suggest potential benefits of early anticoagulation in this high-risk population and warrant further prospective validation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


