{"title":"The Prognostic Value of Lymphocyte-to-Monocyte Ratio for Long-Term Survival After TACE in Intermediate-to-Advanced Hepatocellular Carcinoma.","authors":"JingXin Du, WenLong Yang, RuiJiang Liu, Ping Xie","doi":"10.2147/JHC.S555351","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To investigate the predictive value of the preoperative lymphocyte-to-monocyte ratio (LMR) for long-term survival in patients with intermediate-to-advanced hepatocellular carcinoma (HCC) undergoing transarterial chemoembolization (TACE), providing a reference for precise clinical decision-making.</p><p><strong>Patients and methods: </strong>A retrospective analysis was conducted on clinical data from 313 patients with intermediate-to-advanced HCC treated with TACE at Sichuan Provincial People's Hospital between February 2016 and September 2021. Cox regression analysis was used to identify independent risk factors affecting overall survival (OS). The optimal cut-off value for LMR was determined using receiver operating characteristic (ROC) curve analysis. Survival curves were generated using the Kaplan-Meier method, and differences between groups were compared using the Log rank test.</p><p><strong>Results: </strong>Univariate and multivariate regression analyses revealed that LMR (P=0.033), alpha-fetoprotein (AFP, P=0.007), tumor number (P=0.044), BCLC stage (P=0.013), systemic immune-inflammation index (SII, P=0.044), and fibrosis-4 index (FIB-4, P=0.040) were independent risk factors for OS. Kaplan-Meier survival analysis further demonstrated that, in addition to LMR, patients with AFP > 642.08 ng/mL, cholinesterase ≤ 4.55 kU/L, SII > 250.91, neutrophil-to-lymphocyte ratio (NLR) > 2.85, and FIB-4 > 4.51 also exhibited significantly lower survival rates (all P < 0.05). The optimal cut-off value for LMR was 2.71 (AUC=0.62). Patients with LMR ≤ 2.71 had a significantly lower 3-year survival rate (23.8%) compared to those with LMR > 2.71 (54.2%; log-rank χ² = 21.2, P<0.001).</p><p><strong>Conclusion: </strong>This study confirms that pre-treatment LMR is an independent predictor of overall survival following TACE in a cohort predominantly composed of patients with intermediate-to-advanced HCC classified as BCLC stage C. LMR may serve as a valuable complement to traditional prognostic models, providing incremental value for prognostic assessment in this specific patient population.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"2225-2233"},"PeriodicalIF":3.4000,"publicationDate":"2025-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12499595/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S555351","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To investigate the predictive value of the preoperative lymphocyte-to-monocyte ratio (LMR) for long-term survival in patients with intermediate-to-advanced hepatocellular carcinoma (HCC) undergoing transarterial chemoembolization (TACE), providing a reference for precise clinical decision-making.
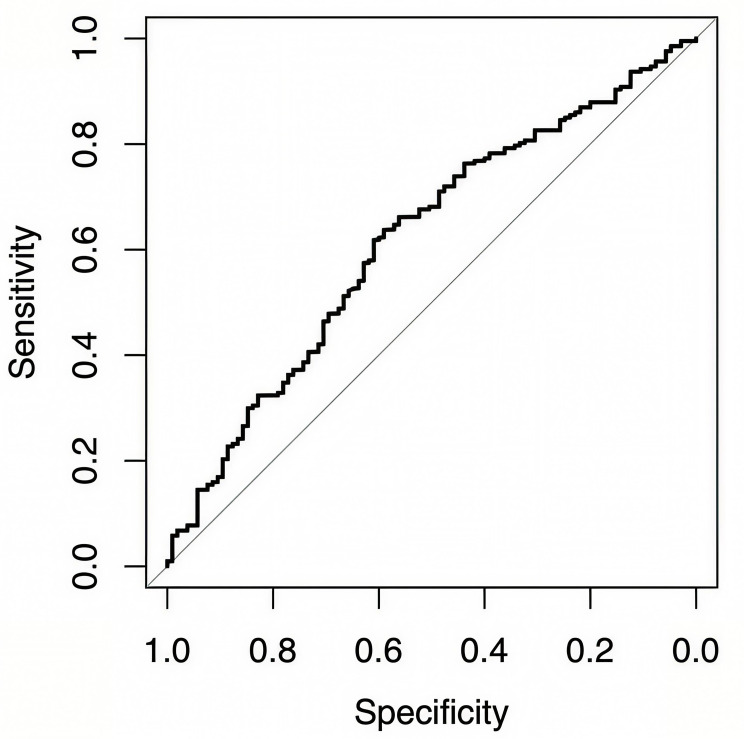
Patients and methods: A retrospective analysis was conducted on clinical data from 313 patients with intermediate-to-advanced HCC treated with TACE at Sichuan Provincial People's Hospital between February 2016 and September 2021. Cox regression analysis was used to identify independent risk factors affecting overall survival (OS). The optimal cut-off value for LMR was determined using receiver operating characteristic (ROC) curve analysis. Survival curves were generated using the Kaplan-Meier method, and differences between groups were compared using the Log rank test.
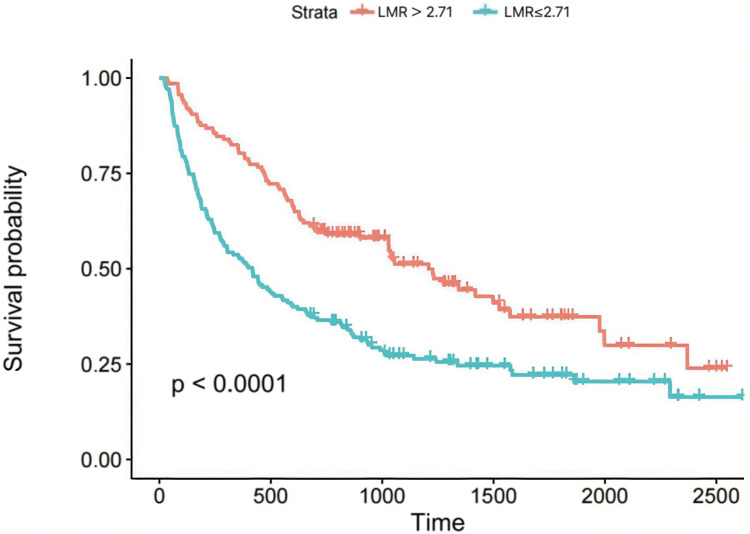
Results: Univariate and multivariate regression analyses revealed that LMR (P=0.033), alpha-fetoprotein (AFP, P=0.007), tumor number (P=0.044), BCLC stage (P=0.013), systemic immune-inflammation index (SII, P=0.044), and fibrosis-4 index (FIB-4, P=0.040) were independent risk factors for OS. Kaplan-Meier survival analysis further demonstrated that, in addition to LMR, patients with AFP > 642.08 ng/mL, cholinesterase ≤ 4.55 kU/L, SII > 250.91, neutrophil-to-lymphocyte ratio (NLR) > 2.85, and FIB-4 > 4.51 also exhibited significantly lower survival rates (all P < 0.05). The optimal cut-off value for LMR was 2.71 (AUC=0.62). Patients with LMR ≤ 2.71 had a significantly lower 3-year survival rate (23.8%) compared to those with LMR > 2.71 (54.2%; log-rank χ² = 21.2, P<0.001).
Conclusion: This study confirms that pre-treatment LMR is an independent predictor of overall survival following TACE in a cohort predominantly composed of patients with intermediate-to-advanced HCC classified as BCLC stage C. LMR may serve as a valuable complement to traditional prognostic models, providing incremental value for prognostic assessment in this specific patient population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


