Haley Bento, Deborah Slay, Maxwell Hunter, Bryan Lohse, Zhining Ou, Angela P Presson, Margaret A French
{"title":"Reducing Upper Extremity Precautions After Lung Transplant: The Clamshell Protocol Pilot Study.","authors":"Haley Bento, Deborah Slay, Maxwell Hunter, Bryan Lohse, Zhining Ou, Angela P Presson, Margaret A French","doi":"10.1097/CPT.0000000000000300","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>A less-restrictive clamshell precaution (CP) protocol for postsurgical upper extremity (UE) movement was implemented after lung transplantation (LTx) instead of traditional sternal precaution (SP) protocols. The purpose of this pilot study is to assess the safety of transitioning from the SP protocol to the CP protocol.</p><p><strong>Methods: </strong>This pilot study was a single-site, observational, cohort study at an academic medical center from March 1, 2021, to February 28, 2023. The CP protocol was implemented on March 1, 2022. Cohorts were determined by the protocol in place at the date of LTx. Safety is described by the frequency of adverse events (AEs), defined as sternal instability or chronic surgical wound infection within 6 months. Summary statistics were reported. Adverse event rates are reported with 95% Wilson score confidence intervals (CIs).</p><p><strong>Results: </strong>Demographics and clinical characteristics were similar between the cohorts. AEs occurred in 4 patients (10%), including 3 patients (18.8%, 95% CI: 6.6%-43.0%) in the SP cohort (n = 16) and 1 patient (4.2%, 95% CI: 0.7%-20.2%) in the CP cohort (n = 24). Those with AEs were older with a higher body mass index and comorbidity index score compared with those who did not have AEs.</p><p><strong>Discussion: </strong>In this pilot study of reducing UE movement restrictions after LTx, there was preliminary evidence of lower AEs, suggesting that reducing restrictions may be a safe alternative to the current standard of care.</p><p><strong>Conclusions: </strong>The results of this pilot study provide preliminary support for the safety CP protocol. However, because of the small sample sizes, further studies are needed to confirm this.</p>","PeriodicalId":72526,"journal":{"name":"Cardiopulmonary physical therapy journal","volume":"36 4","pages":"243-249"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12490332/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiopulmonary physical therapy journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CPT.0000000000000300","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: A less-restrictive clamshell precaution (CP) protocol for postsurgical upper extremity (UE) movement was implemented after lung transplantation (LTx) instead of traditional sternal precaution (SP) protocols. The purpose of this pilot study is to assess the safety of transitioning from the SP protocol to the CP protocol.
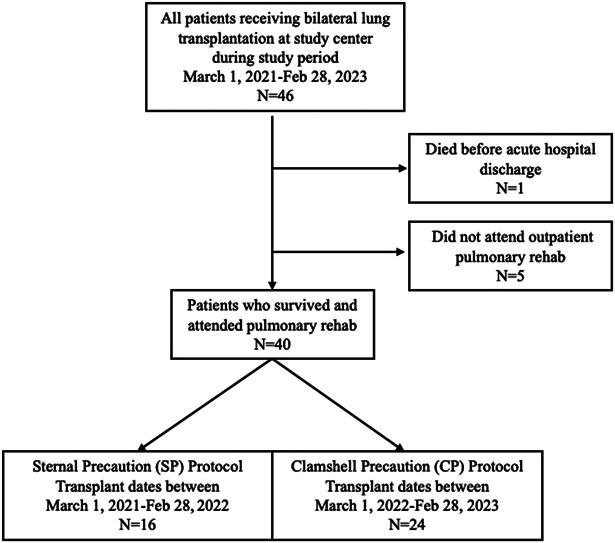
Methods: This pilot study was a single-site, observational, cohort study at an academic medical center from March 1, 2021, to February 28, 2023. The CP protocol was implemented on March 1, 2022. Cohorts were determined by the protocol in place at the date of LTx. Safety is described by the frequency of adverse events (AEs), defined as sternal instability or chronic surgical wound infection within 6 months. Summary statistics were reported. Adverse event rates are reported with 95% Wilson score confidence intervals (CIs).
Results: Demographics and clinical characteristics were similar between the cohorts. AEs occurred in 4 patients (10%), including 3 patients (18.8%, 95% CI: 6.6%-43.0%) in the SP cohort (n = 16) and 1 patient (4.2%, 95% CI: 0.7%-20.2%) in the CP cohort (n = 24). Those with AEs were older with a higher body mass index and comorbidity index score compared with those who did not have AEs.
Discussion: In this pilot study of reducing UE movement restrictions after LTx, there was preliminary evidence of lower AEs, suggesting that reducing restrictions may be a safe alternative to the current standard of care.
Conclusions: The results of this pilot study provide preliminary support for the safety CP protocol. However, because of the small sample sizes, further studies are needed to confirm this.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


