Cherri Zhang, Niranjan Kissoon, J Mark Ansermino, Vuong Nguyen, Elias Kumbakumba, Stephen Businge, Abner Tagoola, Nathan Kenya-Mugisha, Jerome Kabakyenga, Matthew O Wiens
{"title":"Diverging pathways: exploring the interplay between hospital readmission and postdischarge mortality in paediatric sepsis in low-income settings.","authors":"Cherri Zhang, Niranjan Kissoon, J Mark Ansermino, Vuong Nguyen, Elias Kumbakumba, Stephen Businge, Abner Tagoola, Nathan Kenya-Mugisha, Jerome Kabakyenga, Matthew O Wiens","doi":"10.1136/bmjgh-2025-020128","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mortality and readmission rates are high in low-income countries following hospital discharge; however, few studies have studied the relationship between these outcomes. Hospital readmission is a complex outcome as it reflects illness severity and health-seeking behaviour. This study aims to better understand the heterogeneous nature of hospital readmission, especially as it pertains to mortality.</p><p><strong>Methods: </strong>Secondary analysis of a prospective, multisite, observational cohort study included children aged 0-60 months old admitted to hospital with suspected sepsis. We used Fine-Gray models and Cox proportional hazards regression to identify and contrast risk factors for readmission and postdischarge mortality. We also compared the risk ratio of the two outcomes across several domains, including diagnosis, postdischarge time period and study site.</p><p><strong>Results: </strong>Of 6074 children discharged, 376 (6.2%) died, while 1106 (18.2%) were readmitted shortly after discharge. The median time to death and readmission was 28 (IQR: 9-74) and 79.5 (IQR: 30-130) days, respectively. A few patient characteristics, such as prior care seeking and hypoxaemia, were associated with both mortality and readmission. However, other characteristics, such as malnutrition (adjusted HR (aHR): 5.58 (95% CI: 4.20 to 7.43)), HIV (aHR: 1.89 (95% CI: 1.20 to 2.98)) and unplanned discharge (aHR: 3.31 (95% CI: 2.61 to 4.21)), were strongly predictive of postdischarge mortality but not readmission (aSHR: 0.67 (95% CI: 0.56 to 0.81), 0.64 (95% CI: 0.40 to 1.00) and 0.81 (95% CI: 0.67 to 0.98), respectively). The overall rate ratio of readmission to postdischarge mortality was 3.12 (95% CI: 2.77 to 3.50) and increased over time, mostly due to decreasing mortality.</p><p><strong>Conclusions: </strong>Readmission as an outcome measure reflects perceived illness severity, health system capacity and complex healthcare-seeking behaviour. Unlike mortality, readmission is not a reliable surrogate for recurrent illness and should not be used as a primary measure of impact for programmes aiming to improve postdischarge outcomes.</p>","PeriodicalId":9137,"journal":{"name":"BMJ Global Health","volume":"10 10","pages":""},"PeriodicalIF":6.1000,"publicationDate":"2025-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12496109/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Global Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjgh-2025-020128","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Mortality and readmission rates are high in low-income countries following hospital discharge; however, few studies have studied the relationship between these outcomes. Hospital readmission is a complex outcome as it reflects illness severity and health-seeking behaviour. This study aims to better understand the heterogeneous nature of hospital readmission, especially as it pertains to mortality.
Methods: Secondary analysis of a prospective, multisite, observational cohort study included children aged 0-60 months old admitted to hospital with suspected sepsis. We used Fine-Gray models and Cox proportional hazards regression to identify and contrast risk factors for readmission and postdischarge mortality. We also compared the risk ratio of the two outcomes across several domains, including diagnosis, postdischarge time period and study site.
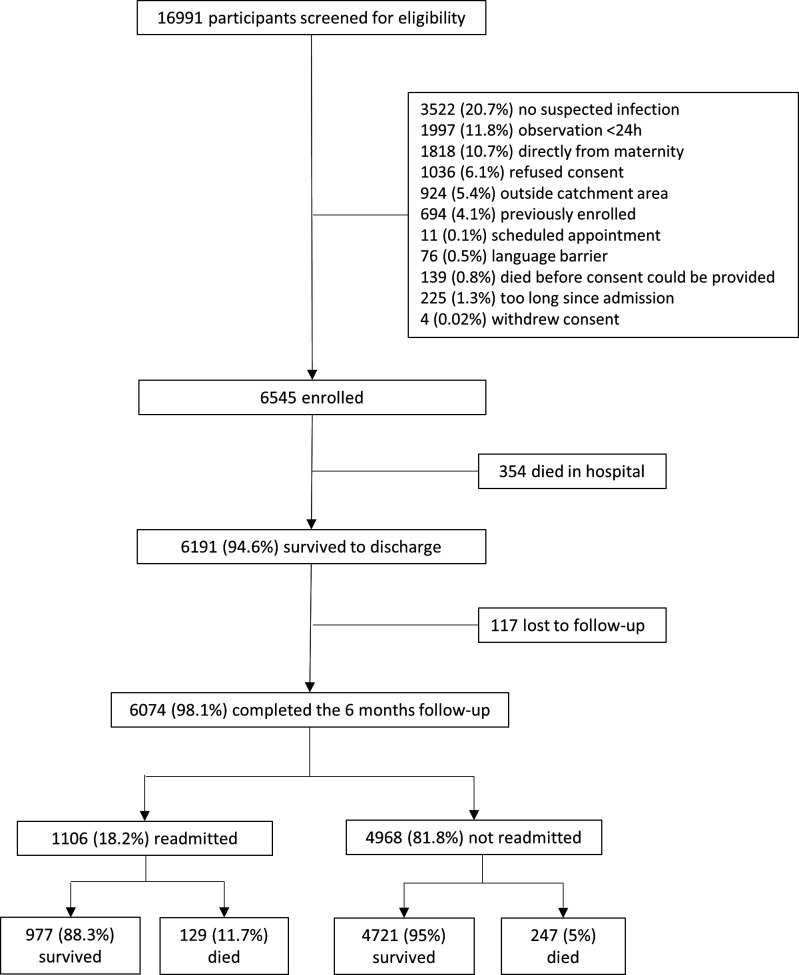
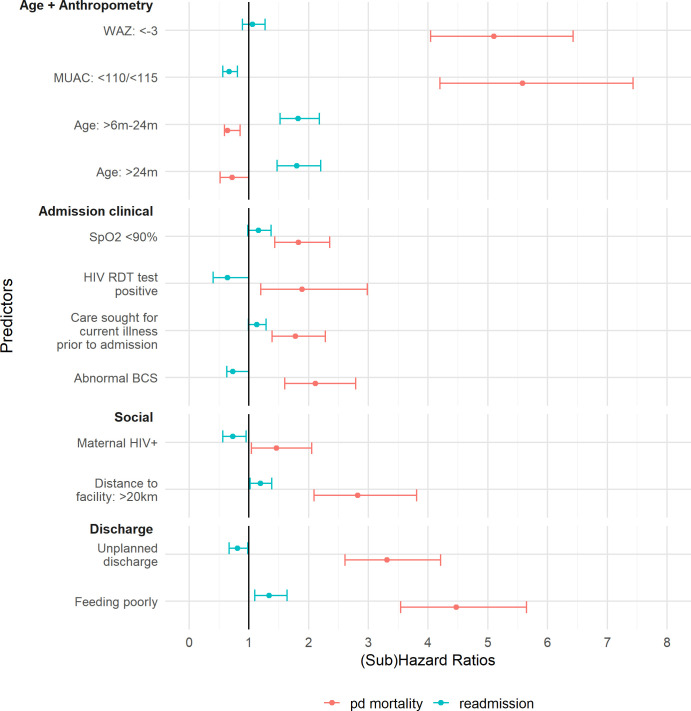
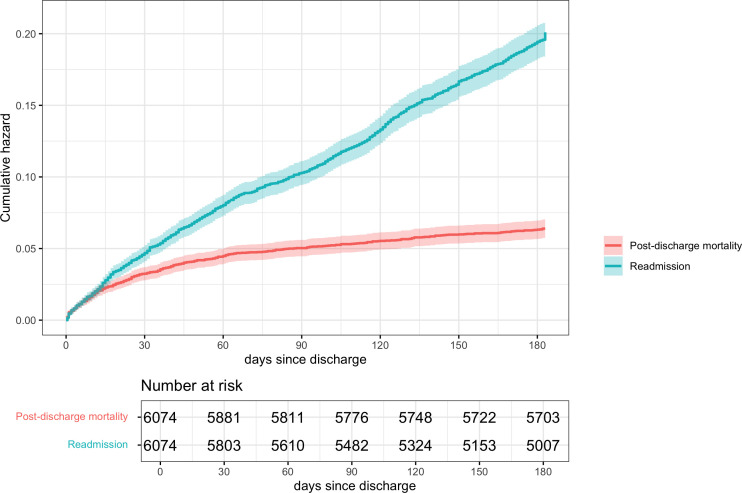
Results: Of 6074 children discharged, 376 (6.2%) died, while 1106 (18.2%) were readmitted shortly after discharge. The median time to death and readmission was 28 (IQR: 9-74) and 79.5 (IQR: 30-130) days, respectively. A few patient characteristics, such as prior care seeking and hypoxaemia, were associated with both mortality and readmission. However, other characteristics, such as malnutrition (adjusted HR (aHR): 5.58 (95% CI: 4.20 to 7.43)), HIV (aHR: 1.89 (95% CI: 1.20 to 2.98)) and unplanned discharge (aHR: 3.31 (95% CI: 2.61 to 4.21)), were strongly predictive of postdischarge mortality but not readmission (aSHR: 0.67 (95% CI: 0.56 to 0.81), 0.64 (95% CI: 0.40 to 1.00) and 0.81 (95% CI: 0.67 to 0.98), respectively). The overall rate ratio of readmission to postdischarge mortality was 3.12 (95% CI: 2.77 to 3.50) and increased over time, mostly due to decreasing mortality.
Conclusions: Readmission as an outcome measure reflects perceived illness severity, health system capacity and complex healthcare-seeking behaviour. Unlike mortality, readmission is not a reliable surrogate for recurrent illness and should not be used as a primary measure of impact for programmes aiming to improve postdischarge outcomes.
期刊介绍:
BMJ Global Health is an online Open Access journal from BMJ that focuses on publishing high-quality peer-reviewed content pertinent to individuals engaged in global health, including policy makers, funders, researchers, clinicians, and frontline healthcare workers. The journal encompasses all facets of global health, with a special emphasis on submissions addressing underfunded areas such as non-communicable diseases (NCDs). It welcomes research across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialized studies. The journal also encourages opinionated discussions on controversial topics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


