Biswadev Mitra, Michael C Reade, Steve Bernard, Bridget Dicker, Marc Maegele, Russell L Gruen
{"title":"High ratio of plasma to red cells in contemporary resuscitation of haemorrhagic shock after trauma: a secondary analysis of the PATCH-trauma trial.","authors":"Biswadev Mitra, Michael C Reade, Steve Bernard, Bridget Dicker, Marc Maegele, Russell L Gruen","doi":"10.1186/s13049-025-01476-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Plasma transfusion is recommended as an initial intervention in most major haemorrhage protocols for trauma resuscitation. With availability of newer blood components, therapeutic agents and investigations for coagulopathy, the marginal benefits of high ratios of plasma to red cells is uncertain. The aim of this study was to report the association of high ratios of plasma: red cells and 28-day mortality in patients with major trauma.</p><p><strong>Methods: </strong>The PATCH-Trauma trial enrolled critically bleeding patients at high risk of trauma induced coagulopathy and randomised them to receive prehospital tranexamic acid or placebo. The sub-group of patients who were managed with massive transfusions in hospital (> 4 units of red cells in first 4 h) were included for this post-hoc analysis. Associations of high ratios of plasma (more than 1 unit of plasma for every 2 units of red cells) and 28-day mortality were reported using multivariable logistic regression analysis after adjustment for potential confounders including age, neurological injury, injury severity, coagulopathy and administration of platelets, fibrinogen concentrates, cryoprecipitate and tranexamic acid.</p><p><strong>Results: </strong>Among 1310 patients enrolled in the PATCH-trauma trial, 372 patients were included for this analysis; 213 (57.3%) received high ratios of plasma: red cells and 116 (31.4%) deaths were recorded at 28 days. High ratios of plasma: red cells were associated with lower mortality (adjusted odds ratio; aOR 0.50; 95%CI: 0.26-0.96). Older age (aOR 1.02; 95%CI: 1.01-1.03), initial Glasgow Coma Scale 3-8 (aOR 6.57; 95%CI: 2.92-14.80) and trauma induced coagulopathy (aOR 5.64; 95%CI: 2.87-11.1) on hospital arrival were associated with higher mortality.</p><p><strong>Conclusions: </strong>Among patients with critical bleeding managed with massive transfusions, high ratios of plasma: red cells were associated with lower mortality, after controlling for potential confounders. Ongoing provision of early plasma for management of critical bleeding is indicated with consideration to prehospital plasma.</p><p><strong>Registration: </strong>ClinicalTrials.gov number, NCT02187120 (Registered 09 July 2014).</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"154"},"PeriodicalIF":3.1000,"publicationDate":"2025-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12492629/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01476-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Plasma transfusion is recommended as an initial intervention in most major haemorrhage protocols for trauma resuscitation. With availability of newer blood components, therapeutic agents and investigations for coagulopathy, the marginal benefits of high ratios of plasma to red cells is uncertain. The aim of this study was to report the association of high ratios of plasma: red cells and 28-day mortality in patients with major trauma.
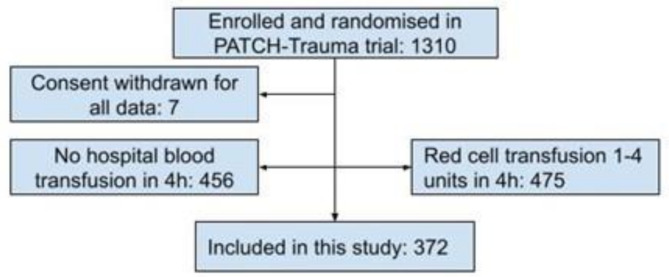
Methods: The PATCH-Trauma trial enrolled critically bleeding patients at high risk of trauma induced coagulopathy and randomised them to receive prehospital tranexamic acid or placebo. The sub-group of patients who were managed with massive transfusions in hospital (> 4 units of red cells in first 4 h) were included for this post-hoc analysis. Associations of high ratios of plasma (more than 1 unit of plasma for every 2 units of red cells) and 28-day mortality were reported using multivariable logistic regression analysis after adjustment for potential confounders including age, neurological injury, injury severity, coagulopathy and administration of platelets, fibrinogen concentrates, cryoprecipitate and tranexamic acid.
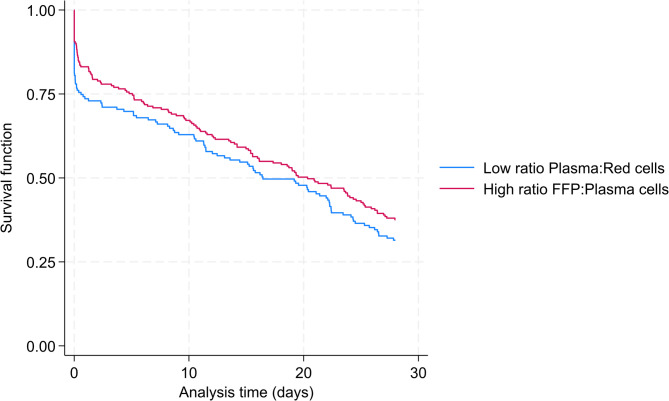
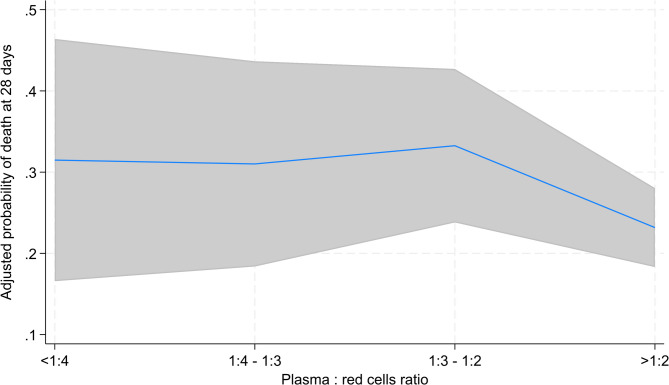
Results: Among 1310 patients enrolled in the PATCH-trauma trial, 372 patients were included for this analysis; 213 (57.3%) received high ratios of plasma: red cells and 116 (31.4%) deaths were recorded at 28 days. High ratios of plasma: red cells were associated with lower mortality (adjusted odds ratio; aOR 0.50; 95%CI: 0.26-0.96). Older age (aOR 1.02; 95%CI: 1.01-1.03), initial Glasgow Coma Scale 3-8 (aOR 6.57; 95%CI: 2.92-14.80) and trauma induced coagulopathy (aOR 5.64; 95%CI: 2.87-11.1) on hospital arrival were associated with higher mortality.
Conclusions: Among patients with critical bleeding managed with massive transfusions, high ratios of plasma: red cells were associated with lower mortality, after controlling for potential confounders. Ongoing provision of early plasma for management of critical bleeding is indicated with consideration to prehospital plasma.
Registration: ClinicalTrials.gov number, NCT02187120 (Registered 09 July 2014).
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


