{"title":"The impact of different neoadjuvant radiotherapy doses on survival outcomes and toxicity in patients with locally advanced rectal cancer.","authors":"Weiting Huang, Xuming Duan, Hujian Hong, Yan Li, Yongyan Shen, Deyu Sun, Yanli Qu","doi":"10.1186/s13014-025-02726-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>To investigate the impact of two neoadjuvant radiotherapy regimens on survival outcomes and adverse reactions in patients with locally advanced low and mid rectal cancer.</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 247 patients with locally advanced rectal cancer, treated at the Department of Radiation Oncology, Liaoning Cancer Hospital, between January 2015 and December 2020. The patients received two different neoadjuvant radiotherapy regimens: In the experimental group, the prescribed radiation dose for the primary rectal tumor and metastatic lymph nodes (PGTV) was 50.4 Gy/24 fractions, and for the pelvic lymphatic drainage area (PTV) was 45.6 Gy/24 fractions. In the control group, the prescribed radiation dose for the rectal tumor and pelvic lymphatic drainage area (PTV) was 50 Gy/25 fractions. The primary endpoints of the study included comparing the two groups in terms of pathological complete response (pCR), anal sphincter preservation rate, 3-year overall survival (OS), 3-year progression-free survival (PFS), acute adverse reactions, perioperative complications, preventive ileostomy reversal rate after LAR, and late adverse reactions. The secondary endpoints included comparing tumor regression grade (TRG), pT downstaging rate, pN downstaging rate, 3-year disease-free survival (DFS), 3-year metastasis-free survival (MFS), and 3-year local recurrence-free survival (LRFS) between the two groups. Univariate and multivariate analyses were performed to identify clinical factors influencing prognosis.</p><p><strong>Results: </strong>This study included 247 patients with locally advanced rectal cancer, all of whom underwent synchronous chemoradiotherapy and radical total mesorectal excision (TME). The experimental group showed comparable results to the control group in terms of pCR rate, anal sphincter preservation rate, TRG grade, pT and pN downstaging rates, as well as 3-year OS, PFS, DFS, MFS, and LRFS (P > 0.05). The experimental group exhibited a significantly lower incidence of ≥ 3 grade acute adverse reactions compared to the control group and had no severe adverse events leading to perioperative mortality. Additionally, the experimental group showed a significantly lower incidence of perioperative complications and a higher preventive ileostomy reversal rate. There were no significant differences between the groups in the incidence of ≥ 3 grade late adverse reactions. Univariate analysis revealed that gender, TRG grade, postoperative T/N stage, cancer nodules, and baseline CEA and CA199 levels were significant factors influencing OS, PFS, DFS, MFS, and LRFS. Multivariate analysis indicated that postoperative T stage, N stage, and baseline CA199 were significantly correlated with OS, PFS, DFS, and MFS, while postoperative T stage was significantly associated with LRFS.</p><p><strong>Conclusions: </strong>Compared to the control group, the experimental group, which utilized a reduced radiation dose for the pelvic lymphatic drainage area, achieved a significantly lower incidence of ≥ 3 grade acute adverse reactions, fewer perioperative complications, and a higher preventive ileostomy reversal rate without any severe perioperative mortality, thereby enhancing the patients' quality of life, without compromising short-term efficacy or survival outcomes.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"20 1","pages":"143"},"PeriodicalIF":3.3000,"publicationDate":"2025-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12482401/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-025-02726-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: To investigate the impact of two neoadjuvant radiotherapy regimens on survival outcomes and adverse reactions in patients with locally advanced low and mid rectal cancer.
Methods: A retrospective analysis was conducted on 247 patients with locally advanced rectal cancer, treated at the Department of Radiation Oncology, Liaoning Cancer Hospital, between January 2015 and December 2020. The patients received two different neoadjuvant radiotherapy regimens: In the experimental group, the prescribed radiation dose for the primary rectal tumor and metastatic lymph nodes (PGTV) was 50.4 Gy/24 fractions, and for the pelvic lymphatic drainage area (PTV) was 45.6 Gy/24 fractions. In the control group, the prescribed radiation dose for the rectal tumor and pelvic lymphatic drainage area (PTV) was 50 Gy/25 fractions. The primary endpoints of the study included comparing the two groups in terms of pathological complete response (pCR), anal sphincter preservation rate, 3-year overall survival (OS), 3-year progression-free survival (PFS), acute adverse reactions, perioperative complications, preventive ileostomy reversal rate after LAR, and late adverse reactions. The secondary endpoints included comparing tumor regression grade (TRG), pT downstaging rate, pN downstaging rate, 3-year disease-free survival (DFS), 3-year metastasis-free survival (MFS), and 3-year local recurrence-free survival (LRFS) between the two groups. Univariate and multivariate analyses were performed to identify clinical factors influencing prognosis.
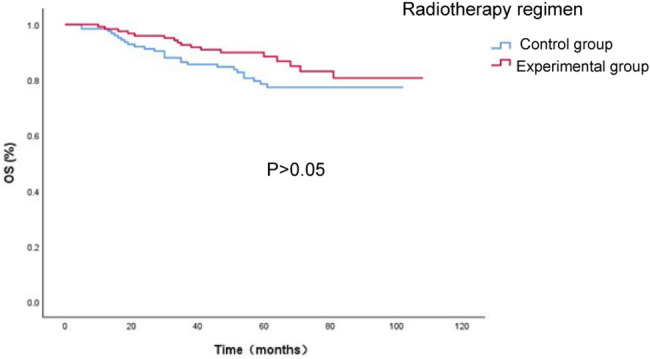
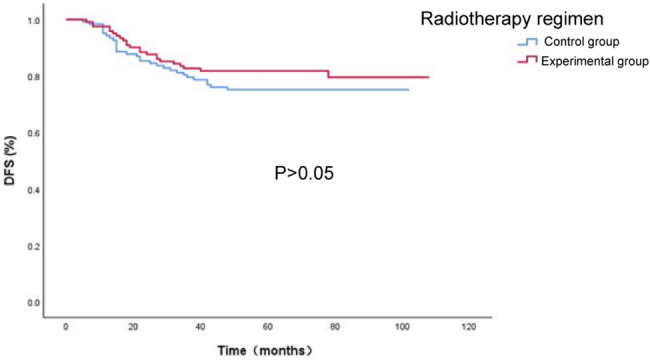
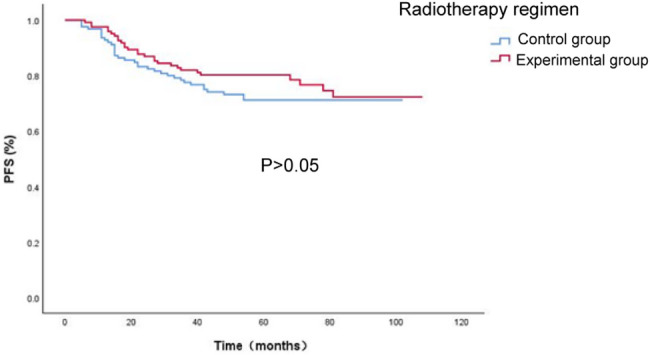
Results: This study included 247 patients with locally advanced rectal cancer, all of whom underwent synchronous chemoradiotherapy and radical total mesorectal excision (TME). The experimental group showed comparable results to the control group in terms of pCR rate, anal sphincter preservation rate, TRG grade, pT and pN downstaging rates, as well as 3-year OS, PFS, DFS, MFS, and LRFS (P > 0.05). The experimental group exhibited a significantly lower incidence of ≥ 3 grade acute adverse reactions compared to the control group and had no severe adverse events leading to perioperative mortality. Additionally, the experimental group showed a significantly lower incidence of perioperative complications and a higher preventive ileostomy reversal rate. There were no significant differences between the groups in the incidence of ≥ 3 grade late adverse reactions. Univariate analysis revealed that gender, TRG grade, postoperative T/N stage, cancer nodules, and baseline CEA and CA199 levels were significant factors influencing OS, PFS, DFS, MFS, and LRFS. Multivariate analysis indicated that postoperative T stage, N stage, and baseline CA199 were significantly correlated with OS, PFS, DFS, and MFS, while postoperative T stage was significantly associated with LRFS.
Conclusions: Compared to the control group, the experimental group, which utilized a reduced radiation dose for the pelvic lymphatic drainage area, achieved a significantly lower incidence of ≥ 3 grade acute adverse reactions, fewer perioperative complications, and a higher preventive ileostomy reversal rate without any severe perioperative mortality, thereby enhancing the patients' quality of life, without compromising short-term efficacy or survival outcomes.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


