{"title":"Strategies for discontinuing vasopressin and norepinephrine during the recovery phase of shock: a single-center retrospective study.","authors":"Shiho Suganuma, Shigehiko Uchino, Seiya Nishiyama, Yusuke Sasabuchi, Shinshu Katayama","doi":"10.1186/s40560-025-00823-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal strategy for discontinuing arginine vasopressin and norepinephrine in patients recovering from shock remains uncertain. Although prior studies have suggested a higher risk of hypotension when arginine vasopressin is discontinued first, these findings may have been influenced by baseline imbalances and tapering practices. We conducted a retrospective study to evaluate whether the order of discontinuation between arginine vasopressin and norepinephrine was associated with the incidence of hypotension during the recovery phase of shock, with vasopressor end doses converted to norepinephrine equivalents for analysis.</p><p><strong>Methods: </strong>This was a single-center retrospective cohort study of intensive care unit patients with shock who received both arginine vasopressin and norepinephrine from August 2017 to March 2024. Patients were categorized based on whether arginine vasopressin or norepinephrine was discontinued first. The primary outcome was the incidence of hypotension within 24 h of vasopressor cessation, defined as mean arterial pressure < 60 mmHg requiring a ≥ 25% increase in the remaining vasopressor, reinstitution of the stopped agent, or a bolus of ≥ 500 mL crystalloid or 25 g albumin. Overlap weighting using propensity scores was applied to adjust for baseline imbalances both in the overall cohort and in the septic shock subgroup. Propensity scores were estimated using logistic model, including baseline characteristics, hemodynamic parameters, and vasopressor end doses in norepinephrine equivalents.</p><p><strong>Results: </strong>A total of 524 patients were analyzed, with 293 discontinuing AVP first and 231 discontinuing NE first. In the unadjusted cohorts, hypotension occurred in 19% of the AVP-first group and 26% of the NE-first group. After overlap weighting, all baseline covariates were balanced between the groups, and the incidence of hypotension was not significantly different (19% vs 21%, P = 0.59). In the septic shock subgroup (n = 267), the weighted analysis showed no significant difference in the incidence of hypotension between groups.</p><p><strong>Conclusions: </strong>In patients recovering from shock who received both arginine vasopressin and norepinephrine, discontinuing arginine vasopressin first was not associated with a higher risk of hypotension.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"13 1","pages":"52"},"PeriodicalIF":4.7000,"publicationDate":"2025-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12487481/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-025-00823-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The optimal strategy for discontinuing arginine vasopressin and norepinephrine in patients recovering from shock remains uncertain. Although prior studies have suggested a higher risk of hypotension when arginine vasopressin is discontinued first, these findings may have been influenced by baseline imbalances and tapering practices. We conducted a retrospective study to evaluate whether the order of discontinuation between arginine vasopressin and norepinephrine was associated with the incidence of hypotension during the recovery phase of shock, with vasopressor end doses converted to norepinephrine equivalents for analysis.
Methods: This was a single-center retrospective cohort study of intensive care unit patients with shock who received both arginine vasopressin and norepinephrine from August 2017 to March 2024. Patients were categorized based on whether arginine vasopressin or norepinephrine was discontinued first. The primary outcome was the incidence of hypotension within 24 h of vasopressor cessation, defined as mean arterial pressure < 60 mmHg requiring a ≥ 25% increase in the remaining vasopressor, reinstitution of the stopped agent, or a bolus of ≥ 500 mL crystalloid or 25 g albumin. Overlap weighting using propensity scores was applied to adjust for baseline imbalances both in the overall cohort and in the septic shock subgroup. Propensity scores were estimated using logistic model, including baseline characteristics, hemodynamic parameters, and vasopressor end doses in norepinephrine equivalents.
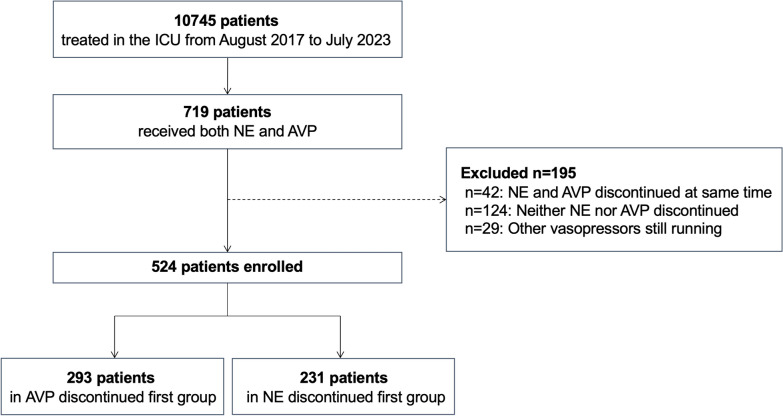
Results: A total of 524 patients were analyzed, with 293 discontinuing AVP first and 231 discontinuing NE first. In the unadjusted cohorts, hypotension occurred in 19% of the AVP-first group and 26% of the NE-first group. After overlap weighting, all baseline covariates were balanced between the groups, and the incidence of hypotension was not significantly different (19% vs 21%, P = 0.59). In the septic shock subgroup (n = 267), the weighted analysis showed no significant difference in the incidence of hypotension between groups.
Conclusions: In patients recovering from shock who received both arginine vasopressin and norepinephrine, discontinuing arginine vasopressin first was not associated with a higher risk of hypotension.
背景:休克恢复期患者停用精氨酸加压素和去甲肾上腺素的最佳策略仍不确定。虽然先前的研究表明,先停用精氨酸抗利尿激素时低血压的风险更高,但这些发现可能受到基线失衡和逐渐减量的影响。我们进行了一项回顾性研究,评估精氨酸加压素和去甲肾上腺素之间的停药顺序是否与休克恢复期低血压的发生率相关,并将加压素结束剂量转换为去甲肾上腺素当量进行分析。方法:对2017年8月至2024年3月同时接受精氨酸加压素和去甲肾上腺素治疗的重症监护病房休克患者进行单中心回顾性队列研究。根据先停用精氨酸抗利尿激素还是去甲肾上腺素对患者进行分类。主要终点是血管加压药停止后24小时内低血压的发生率,定义为平均动脉压。结果:共分析了524例患者,其中293例首先停止AVP治疗,231例首先停止NE治疗。在未调整的队列中,AVP-first组的低血压发生率为19%,NE-first组为26%。重叠加权后,两组间所有基线协变量均平衡,低血压发生率无显著差异(19% vs 21%, P = 0.59)。在脓毒性休克亚组(n = 267),加权分析显示两组间低血压发生率无显著差异。结论:在接受精氨酸加压素和去甲肾上腺素治疗的休克恢复期患者中,首先停用精氨酸加压素与低血压的高风险无关。
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


