Pranav Prakash, Nisarg S, Jayaraj Mymbilly Balakrishnan, Sai Deepak Alli, Ravi G S, Siddhi Rajeev Naik
{"title":"Right ventricular dysfunction: a key predictor of post-intubation hypotension in the emergency department.","authors":"Pranav Prakash, Nisarg S, Jayaraj Mymbilly Balakrishnan, Sai Deepak Alli, Ravi G S, Siddhi Rajeev Naik","doi":"10.1186/s12245-025-00987-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Post-intubation hypotension (PIh) is a frequent complication following drug-assisted intubation, leading to increased morbidity, mortality, and healthcare costs. Pre-intubation hemodynamic factors, acid-base imbalances, and existing comorbidities, particularly right ventricular dysfunction, which is a lesser-known variable, have emerged as a critical predictor of PIh. Since RV systolic motion is predominantly longitudinal, TAPSE on POCUS provides a time-sensitive surrogate of RV function for high risk patients in the Emergency department.</p><p><strong>Methods: </strong>Aim: The study aimed to list hemodynamic predictors and their correlation with easily executable POCUS and point-of-care echocardiography variables, which can impact emergency decision-making and optimal management in PIh. This prospective observational study was conducted in the Department of Emergency Medicine at Kasturba Medical College, Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India. 172 patients aged ≥ 18 years undergoing drug-assisted intubation were observed. Baseline demographics, clinical parameters, hemodynamic indices, and pre-intubation echocardiographic values (TAPSE, EPSS) were recorded. Shock index and modified shock index were calculated. Point-of-care ultrasound (POCUS) assessed left and right ventricular function. PIh within 30 min was defined as SBP [Formula: see text] 90mmHg, ≥ 20% fall in SBP, MAP < 65mmHg or new vasopressor initiation. Associations were tested with logistic regression. TAPSE discrimination was obtained with ROC analysis and Youden's Index.</p><p><strong>Results: </strong>Of the 172 patients, 71 (41.2%) developed PIh. Patients with obstructive lung disease (59.3%, p = 0.039) and sepsis (66.7%) were significantly more likely to experience PIh. TAPSE values were significantly lower in those with PIh (17.66 ± 2.45 mm vs. 18.54 ± 2.15 mm, p = 0.014). The multivariate logistic regression revealed TAPSE as an independent predictor of PIh (OR = 0.81, 95% CI = 0.69-0.95, p = 0.009). ROC analysis of TAPSE showed moderate predictive power (AUC 0.584, 95% CI 0.497-0.672), with a cut-off of 17.6 mm (sensitivity 85.1% and specificity 29.6%).</p><p><strong>Conclusion: </strong>TAPSE measured pre-intubation emerged as a reliable predictor of post-intubation hypotension. Incorporating a rapid assessment of right ventricular function using POCUS into the airway management algorithm provides valuable insights in identifying patients at higher risk of PIh.</p>","PeriodicalId":13967,"journal":{"name":"International Journal of Emergency Medicine","volume":"18 1","pages":"183"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12487513/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12245-025-00987-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
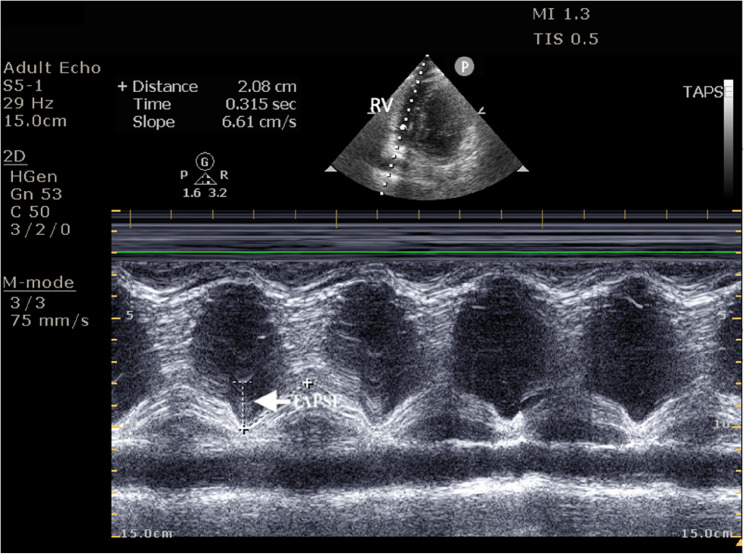
Background: Post-intubation hypotension (PIh) is a frequent complication following drug-assisted intubation, leading to increased morbidity, mortality, and healthcare costs. Pre-intubation hemodynamic factors, acid-base imbalances, and existing comorbidities, particularly right ventricular dysfunction, which is a lesser-known variable, have emerged as a critical predictor of PIh. Since RV systolic motion is predominantly longitudinal, TAPSE on POCUS provides a time-sensitive surrogate of RV function for high risk patients in the Emergency department.
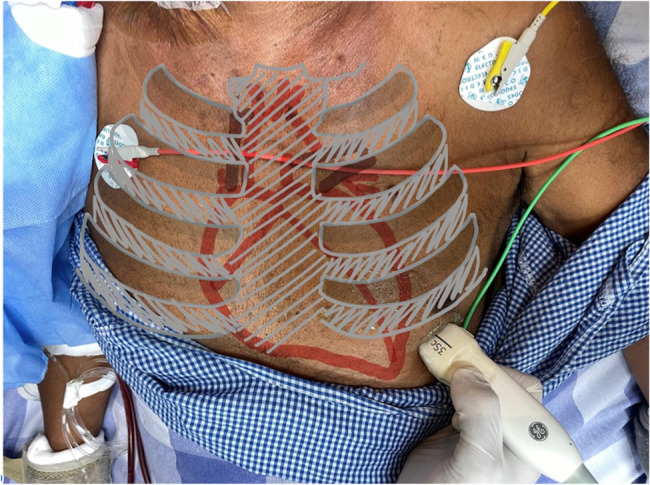
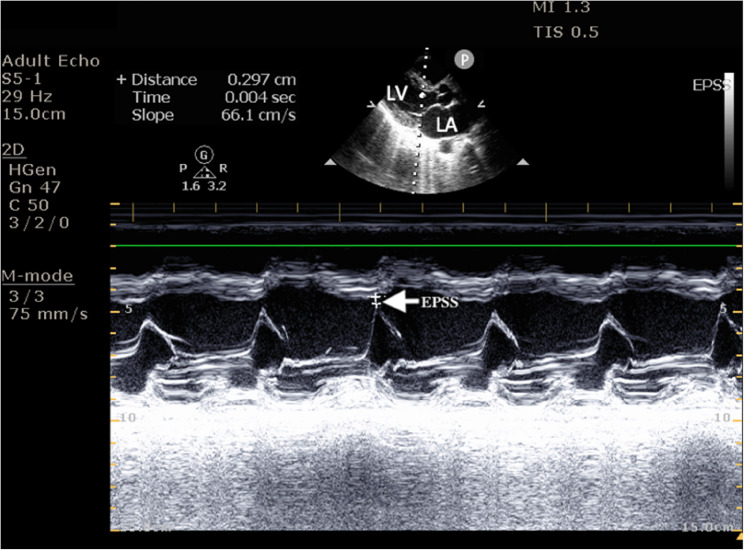
Methods: Aim: The study aimed to list hemodynamic predictors and their correlation with easily executable POCUS and point-of-care echocardiography variables, which can impact emergency decision-making and optimal management in PIh. This prospective observational study was conducted in the Department of Emergency Medicine at Kasturba Medical College, Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India. 172 patients aged ≥ 18 years undergoing drug-assisted intubation were observed. Baseline demographics, clinical parameters, hemodynamic indices, and pre-intubation echocardiographic values (TAPSE, EPSS) were recorded. Shock index and modified shock index were calculated. Point-of-care ultrasound (POCUS) assessed left and right ventricular function. PIh within 30 min was defined as SBP [Formula: see text] 90mmHg, ≥ 20% fall in SBP, MAP < 65mmHg or new vasopressor initiation. Associations were tested with logistic regression. TAPSE discrimination was obtained with ROC analysis and Youden's Index.
Results: Of the 172 patients, 71 (41.2%) developed PIh. Patients with obstructive lung disease (59.3%, p = 0.039) and sepsis (66.7%) were significantly more likely to experience PIh. TAPSE values were significantly lower in those with PIh (17.66 ± 2.45 mm vs. 18.54 ± 2.15 mm, p = 0.014). The multivariate logistic regression revealed TAPSE as an independent predictor of PIh (OR = 0.81, 95% CI = 0.69-0.95, p = 0.009). ROC analysis of TAPSE showed moderate predictive power (AUC 0.584, 95% CI 0.497-0.672), with a cut-off of 17.6 mm (sensitivity 85.1% and specificity 29.6%).
Conclusion: TAPSE measured pre-intubation emerged as a reliable predictor of post-intubation hypotension. Incorporating a rapid assessment of right ventricular function using POCUS into the airway management algorithm provides valuable insights in identifying patients at higher risk of PIh.
背景:插管后低血压(PIh)是药物辅助插管后常见的并发症,导致发病率、死亡率和医疗费用增加。插管前血流动力学因素、酸碱失衡和现有的合并症,特别是鲜为人知的右心室功能障碍,已成为PIh的关键预测因素。由于右心室收缩运动主要是纵向的,在POCUS上的TAPSE为急诊科的高风险患者提供了右心室功能的时间敏感替代品。方法:目的:列出血液动力学预测指标及其与易于执行的POCUS和点位超声心动图变量的相关性,以影响PIh的应急决策和优化管理。本前瞻性观察研究在印度卡纳塔克邦马尼帕尔马尼帕尔高等教育学院Kasturba医学院急诊科进行,观察了172例年龄≥18岁接受药物辅助插管的患者。记录基线人口统计学、临床参数、血流动力学指标和插管前超声心动图值(TAPSE、EPSS)。计算了冲击指数和修正冲击指数。即时超声(POCUS)评估左、右心室功能。30min内的PIh定义为收缩压90mmHg,收缩压下降≥20%,MAP < 65mmHg或新的升压药物启动。用逻辑回归检验相关性。采用ROC分析和约登指数进行TAPSE判别。结果:172例患者中,71例(41.2%)发生PIh。阻塞性肺疾病(59.3%,p = 0.039)和脓毒症(66.7%)患者更容易发生PIh。PIh患者的TAPSE值显著低于前者(17.66±2.45 mm vs. 18.54±2.15 mm, p = 0.014)。多因素logistic回归显示TAPSE是PIh的独立预测因子(OR = 0.81, 95% CI = 0.69-0.95, p = 0.009)。TAPSE的ROC分析显示中等预测能力(AUC 0.584, 95% CI 0.497-0.672),截止值为17.6 mm(敏感性85.1%,特异性29.6%)。结论:插管前测量的TAPSE是插管后低血压的可靠预测指标。将使用POCUS对右心室功能的快速评估纳入气道管理算法,为识别PIh高风险患者提供了有价值的见解。
期刊介绍:
The aim of the journal is to bring to light the various clinical advancements and research developments attained over the world and thus help the specialty forge ahead. It is directed towards physicians and medical personnel undergoing training or working within the field of Emergency Medicine. Medical students who are interested in pursuing a career in Emergency Medicine will also benefit from the journal. This is particularly useful for trainees in countries where the specialty is still in its infancy. Disciplines covered will include interesting clinical cases, the latest evidence-based practice and research developments in Emergency medicine including emergency pediatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


