Development and evaluation of methods of clinical utility-based cut-point selection of diagnostic biomarkers: an analysis based on population-level parametric distributions of test results with application of clinical diagnostic data.
{"title":"Development and evaluation of methods of clinical utility-based cut-point selection of diagnostic biomarkers: an analysis based on population-level parametric distributions of test results with application of clinical diagnostic data.","authors":"Mojtaba Hassanzad, Karimollah Hajian-Tilaki, Zinatossadat Bouzari","doi":"10.1186/s12874-025-02656-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The cut-point selection of biomarkers based on clinical benefit of test results rather than accuracy-based is of interest for decision makers. We adapted the four methods of cut-point selection based on clinical utility of test results including Youden, Product, Union and the absolute difference of total utility with 2 times of AUC.</p><p><strong>Methods: </strong>The population-based parametric pairs of distributions of test results comprising homoscedastic binormal model, non-homoscedastic binormal, bigamma and biexponential included in the study. For each pair of distributions for diseased and non-diseased the utility-based metrics of cut-point were calculated under different degrees of AUC and prevalence. The prevalence was varied from 0.01 to 0.05, 0.10, 0.30, and 0.50.</p><p><strong>Results: </strong>For a low prevalence as low as 0.01, the two methods of Product, and Union that maximize and minimize the related metrics respectively yield rather similar a true value of cut-point but the Youden-based utility metrics suggest rather similarly the true value of for an optimal cut-point. In opposition, the Youden-based utility metric and the absolute difference of total utility with 2 times of AUC produce extremely high value for optimal cut-point because of their s-shaped metrics over various cut-off values. As prevalence increases to 10% or more, the metric of Youden -based utility becomes concave and its cut-point becomes closer to other methods. The four proposed methods yield roughly identical cut-point at prevalence of 10% or more for high accuracy of 0.90. The greater discrepancy of optimal cut-point was shown in skew distributions of bigamma and biexponential with low prevalence and low AUC. For prevalence < 10%, the utility-based produces larger cut-point than accuracy-based methods in our clinical data for CRP. The methods of utility-based cut-point selection were explained by CRP in predicting preeclampsia, and other clinical data.</p><p><strong>Conclusion: </strong>The inconsistency of optimal cut-points is possible by different methods of utility-based criteria depending on the prevalence and degree of AUC. For high AUC, and prevalence > 10%, the four proposed methods yield rather identical optimal cut-points. Further studies of simulation are needed to evaluate the bias and sampling variability of utility-based of cut-point selection.</p>","PeriodicalId":9114,"journal":{"name":"BMC Medical Research Methodology","volume":"25 1","pages":"223"},"PeriodicalIF":3.4000,"publicationDate":"2025-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12482875/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medical Research Methodology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12874-025-02656-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The cut-point selection of biomarkers based on clinical benefit of test results rather than accuracy-based is of interest for decision makers. We adapted the four methods of cut-point selection based on clinical utility of test results including Youden, Product, Union and the absolute difference of total utility with 2 times of AUC.
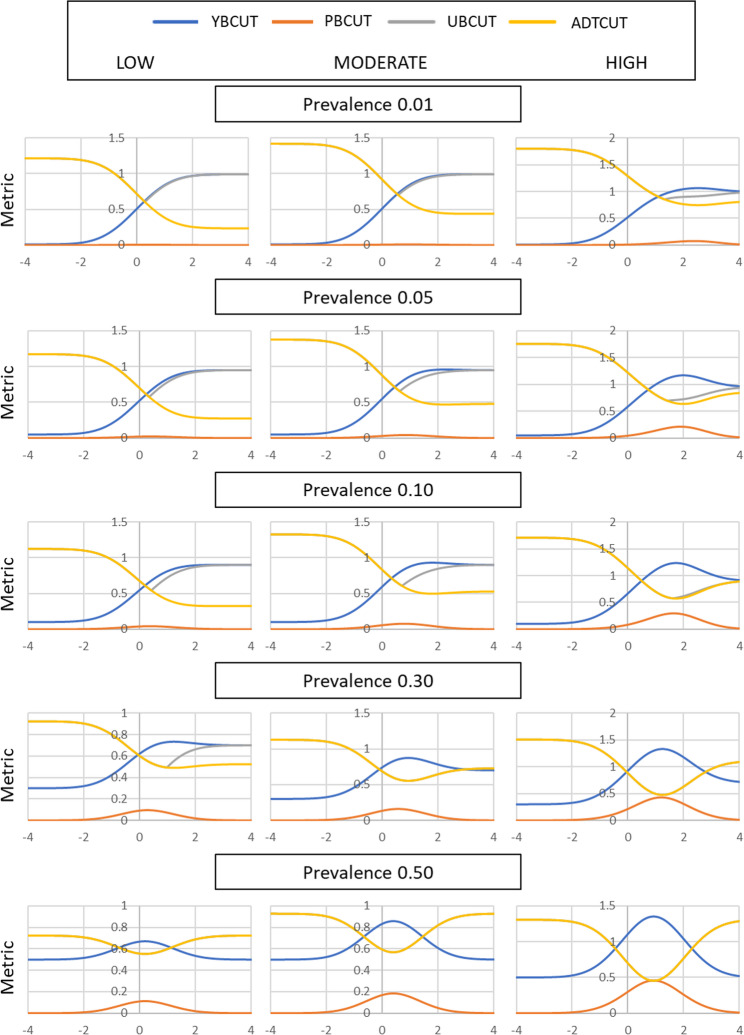
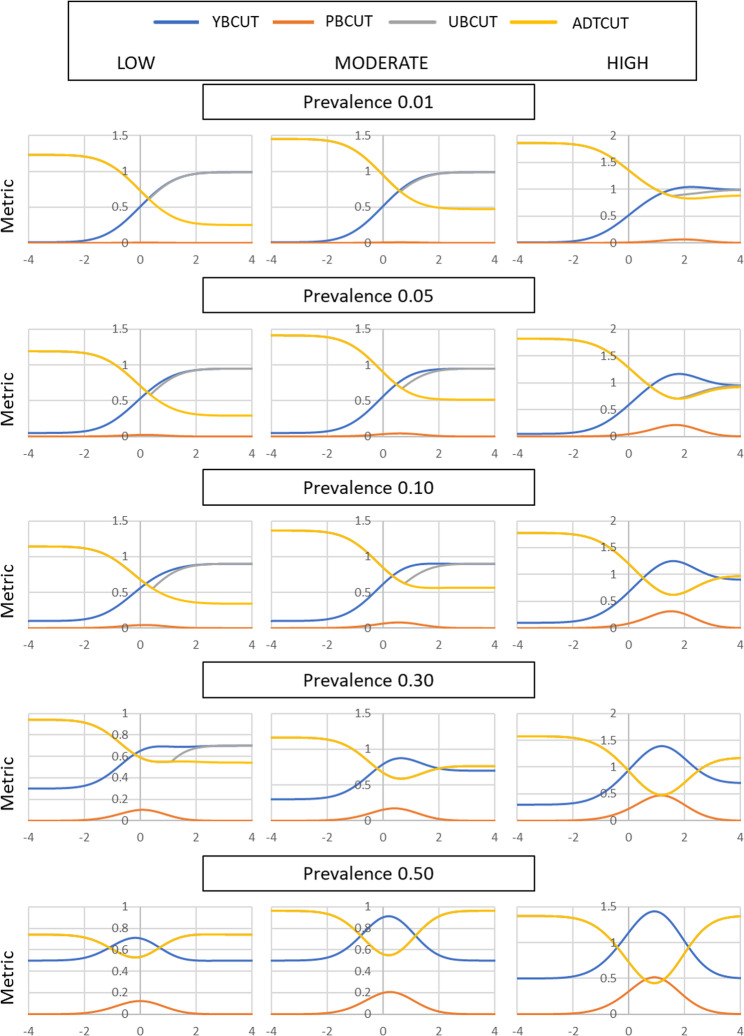
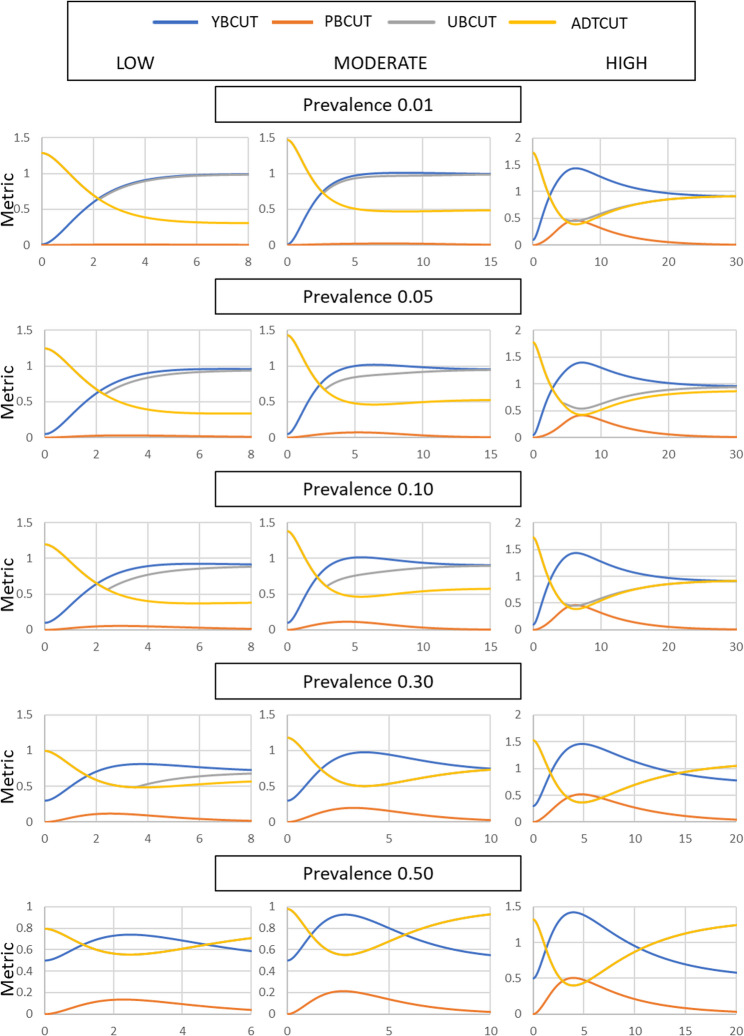
Methods: The population-based parametric pairs of distributions of test results comprising homoscedastic binormal model, non-homoscedastic binormal, bigamma and biexponential included in the study. For each pair of distributions for diseased and non-diseased the utility-based metrics of cut-point were calculated under different degrees of AUC and prevalence. The prevalence was varied from 0.01 to 0.05, 0.10, 0.30, and 0.50.
Results: For a low prevalence as low as 0.01, the two methods of Product, and Union that maximize and minimize the related metrics respectively yield rather similar a true value of cut-point but the Youden-based utility metrics suggest rather similarly the true value of for an optimal cut-point. In opposition, the Youden-based utility metric and the absolute difference of total utility with 2 times of AUC produce extremely high value for optimal cut-point because of their s-shaped metrics over various cut-off values. As prevalence increases to 10% or more, the metric of Youden -based utility becomes concave and its cut-point becomes closer to other methods. The four proposed methods yield roughly identical cut-point at prevalence of 10% or more for high accuracy of 0.90. The greater discrepancy of optimal cut-point was shown in skew distributions of bigamma and biexponential with low prevalence and low AUC. For prevalence < 10%, the utility-based produces larger cut-point than accuracy-based methods in our clinical data for CRP. The methods of utility-based cut-point selection were explained by CRP in predicting preeclampsia, and other clinical data.
Conclusion: The inconsistency of optimal cut-points is possible by different methods of utility-based criteria depending on the prevalence and degree of AUC. For high AUC, and prevalence > 10%, the four proposed methods yield rather identical optimal cut-points. Further studies of simulation are needed to evaluate the bias and sampling variability of utility-based of cut-point selection.
期刊介绍:
BMC Medical Research Methodology is an open access journal publishing original peer-reviewed research articles in methodological approaches to healthcare research. Articles on the methodology of epidemiological research, clinical trials and meta-analysis/systematic review are particularly encouraged, as are empirical studies of the associations between choice of methodology and study outcomes. BMC Medical Research Methodology does not aim to publish articles describing scientific methods or techniques: these should be directed to the BMC journal covering the relevant biomedical subject area.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


