Cameron I Wells, William Xu, Chris Varghese, Sameer Bhat, Wal Baraza, Chris Harmston, Greg O'Grady, Ian P Bissett
{"title":"Definition of failure to rescue in gastrointestinal and hepatobiliary cancer surgery: national cohort study.","authors":"Cameron I Wells, William Xu, Chris Varghese, Sameer Bhat, Wal Baraza, Chris Harmston, Greg O'Grady, Ian P Bissett","doi":"10.1093/bjsopen/zraf116","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Failure to rescue (FTR) is the mortality rate among patients with complications, and is a quality indicator for surgical care. FTR has been inconsistently defined in the literature, with potential impacts on reported rates and hospital benchmarking. This study examined the impact of differences in the FTR definition on hospital rankings.</p><p><strong>Methods: </strong>A retrospective population-based cohort study of patients undergoing gastrointestinal or hepatopancreatobiliary cancer resection from 2005 to 2020 was performed using linkage of the New Zealand Cancer Registry and National Minimum Dataset. FTR was defined as the mortality rate among patients with any of 19 postoperative complications. Five FTR definitions commonly used in the literature were adapted for comparison. Risk-adjusted rates were compared between hospitals using each definition, as well as for in-hospital and 90-day outcomes.</p><p><strong>Results: </strong>In total, 31 199 patients were included from 20 hospitals, with 1517 90-day deaths (4.9%). The 90-day FTR rate with all 19 complications included was 10.4% (1517 of 14 646). The FTR definition affected hospital rankings, with the Bland-Altman 95% limits of agreement ranging between 4 and 11 position differences. There were 847 in-hospital deaths, and the in-hospital FTR rate was 5.8% (847 of 14 516). Hospital rankings were affected by the timing of outcome measurement; 95% limits of agreement ranged from 5 to 8 position differences compared with 90-day outcomes.</p><p><strong>Conclusion: </strong>The definition and timing of FTR measurement affected hospital rankings. This may have important ramifications for FTR as a quality indicator when benchmarking institutional performance.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"9 5","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12481687/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zraf116","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Failure to rescue (FTR) is the mortality rate among patients with complications, and is a quality indicator for surgical care. FTR has been inconsistently defined in the literature, with potential impacts on reported rates and hospital benchmarking. This study examined the impact of differences in the FTR definition on hospital rankings.
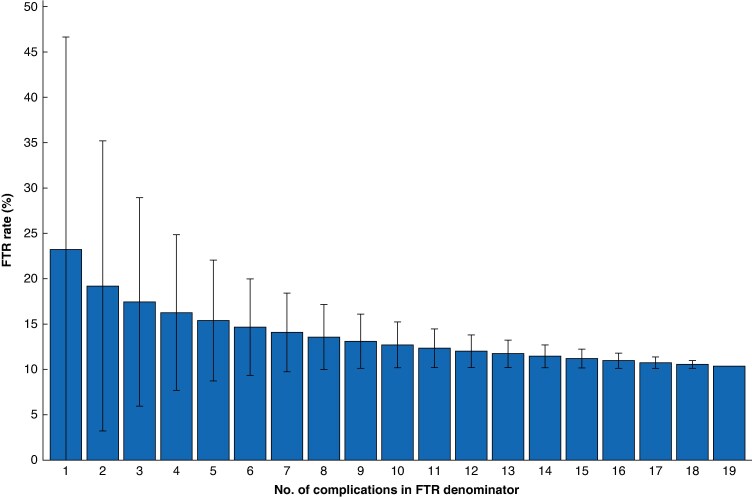
Methods: A retrospective population-based cohort study of patients undergoing gastrointestinal or hepatopancreatobiliary cancer resection from 2005 to 2020 was performed using linkage of the New Zealand Cancer Registry and National Minimum Dataset. FTR was defined as the mortality rate among patients with any of 19 postoperative complications. Five FTR definitions commonly used in the literature were adapted for comparison. Risk-adjusted rates were compared between hospitals using each definition, as well as for in-hospital and 90-day outcomes.
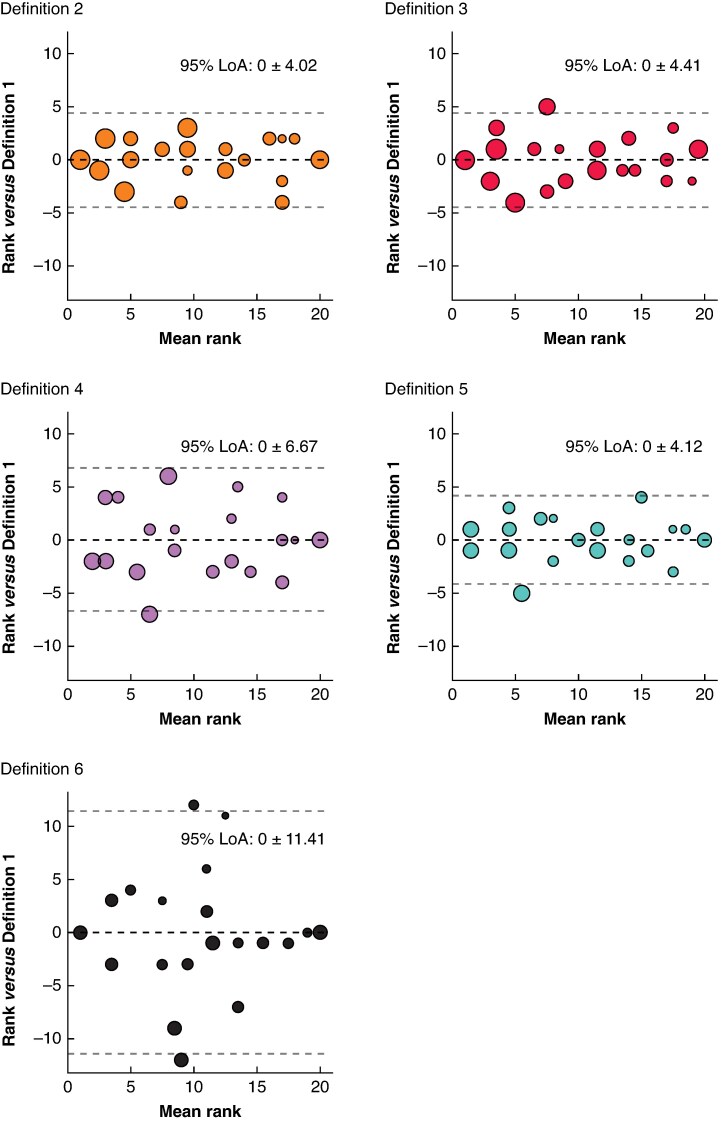
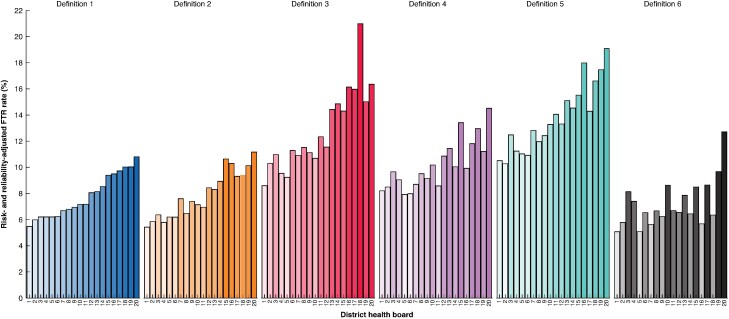
Results: In total, 31 199 patients were included from 20 hospitals, with 1517 90-day deaths (4.9%). The 90-day FTR rate with all 19 complications included was 10.4% (1517 of 14 646). The FTR definition affected hospital rankings, with the Bland-Altman 95% limits of agreement ranging between 4 and 11 position differences. There were 847 in-hospital deaths, and the in-hospital FTR rate was 5.8% (847 of 14 516). Hospital rankings were affected by the timing of outcome measurement; 95% limits of agreement ranged from 5 to 8 position differences compared with 90-day outcomes.
Conclusion: The definition and timing of FTR measurement affected hospital rankings. This may have important ramifications for FTR as a quality indicator when benchmarking institutional performance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


