Reza Khorasanee, Barnaby Sanderson, Emilia Tomarchio, Patrick D Collins, Riccardo Del Signore, Sridevi Shetty, Mara Chioccola, Francesca Pugliese, Francesca Collino, Louise Rose, Lorenzo Giosa, Luigi Camporota
{"title":"Mechanical power normalisation methods to predict ICU mortality: a retrospective cohort study.","authors":"Reza Khorasanee, Barnaby Sanderson, Emilia Tomarchio, Patrick D Collins, Riccardo Del Signore, Sridevi Shetty, Mara Chioccola, Francesca Pugliese, Francesca Collino, Louise Rose, Lorenzo Giosa, Luigi Camporota","doi":"10.1186/s13613-025-01562-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal mechanical ventilation strategy to minimise ventilator-induced lung injury (VILI) remains uncertain. Mechanical power (MP) is a key VILI determinant, but whether and how MP should be normalised to individual patient characteristics is unclear. In this study, we aimed to evaluate whether the discriminatory accuracy of MP for ICU mortality in mechanically ventilated patients improves when normalised to physiologically relevant variables that reflect individual susceptibility to VILI. We also explored whether the relationship between MP, MP<sub>ratio</sub>, and mortality is linear or exhibits a threshold effect.</p><p><strong>Methods: </strong>In this retrospective observational study, we extracted granular electronic healthcare record data for mechanically ventilated adults in a single centre over a seven-year period. Primary exposures were MP with five normalisations: for dead space (expressed as corrected minute ventilation, ventilatory ratio, or end-tidal to arterial CO<sub>2</sub> ratio); aerated lung size (compliance), and normal idealised MP (MP<sub>ratio</sub>). We used logistic regression to assess associations with ICU mortality. We calculated the Area Under the Receiver Operating Characteristic Curve (AUROC) to compare discriminative accuracy of individual models. Additionally, we evaluated the linearity or presence of a threshold for the relationships between MP, MP<sub>ratio</sub> and ICU mortality.</p><p><strong>Result: </strong>We included 3,578 patients in our analyses. We found MP normalised to compliance (AUROC 0.71, 95% confidence interval (CI) 0.69-0.73, p = 0.007 (DeLong's test)) and MP<sub>ratio</sub> (AUROC 0.71, 95% CI 0.68-0.73, p = 0.0014) performed better than MP alone (AUROC 0.69, 95% CI 0.66-0.71) for predicting ICU mortality. Other methods of MP normalisation were no more discriminative than MP without normalisation. The relationship between MP and MP<sub>ratio</sub> with ICU mortality showed a statistically significant but small departure from linearity.</p><p><strong>Conclusions: </strong>Mechanical power normalised to compliance and MP<sub>ratio</sub> had better discrimination for ICU mortality than MP, although the difference was modest and absolute predictive power remained limited.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"149"},"PeriodicalIF":5.5000,"publicationDate":"2025-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12480304/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01562-9","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The optimal mechanical ventilation strategy to minimise ventilator-induced lung injury (VILI) remains uncertain. Mechanical power (MP) is a key VILI determinant, but whether and how MP should be normalised to individual patient characteristics is unclear. In this study, we aimed to evaluate whether the discriminatory accuracy of MP for ICU mortality in mechanically ventilated patients improves when normalised to physiologically relevant variables that reflect individual susceptibility to VILI. We also explored whether the relationship between MP, MPratio, and mortality is linear or exhibits a threshold effect.
Methods: In this retrospective observational study, we extracted granular electronic healthcare record data for mechanically ventilated adults in a single centre over a seven-year period. Primary exposures were MP with five normalisations: for dead space (expressed as corrected minute ventilation, ventilatory ratio, or end-tidal to arterial CO2 ratio); aerated lung size (compliance), and normal idealised MP (MPratio). We used logistic regression to assess associations with ICU mortality. We calculated the Area Under the Receiver Operating Characteristic Curve (AUROC) to compare discriminative accuracy of individual models. Additionally, we evaluated the linearity or presence of a threshold for the relationships between MP, MPratio and ICU mortality.
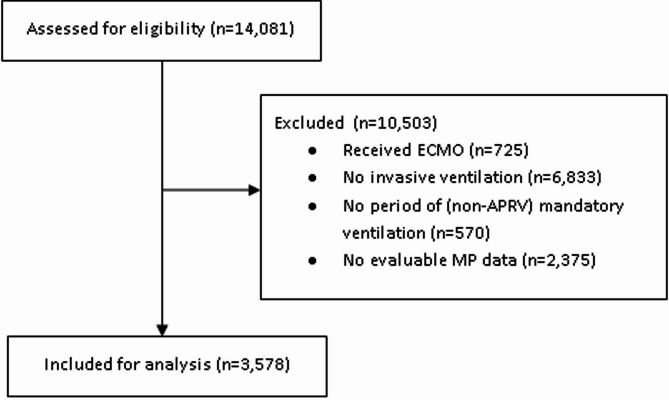
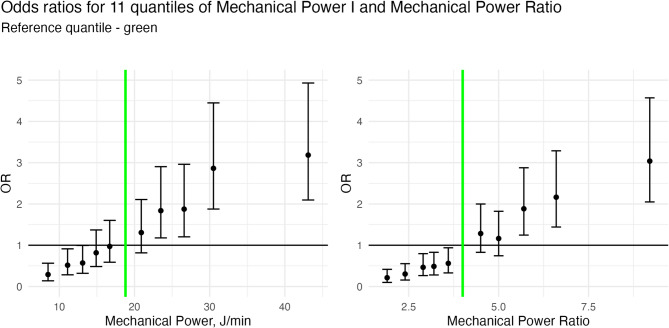
Result: We included 3,578 patients in our analyses. We found MP normalised to compliance (AUROC 0.71, 95% confidence interval (CI) 0.69-0.73, p = 0.007 (DeLong's test)) and MPratio (AUROC 0.71, 95% CI 0.68-0.73, p = 0.0014) performed better than MP alone (AUROC 0.69, 95% CI 0.66-0.71) for predicting ICU mortality. Other methods of MP normalisation were no more discriminative than MP without normalisation. The relationship between MP and MPratio with ICU mortality showed a statistically significant but small departure from linearity.
Conclusions: Mechanical power normalised to compliance and MPratio had better discrimination for ICU mortality than MP, although the difference was modest and absolute predictive power remained limited.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


