Daniel Piñeiro, José Ramón González-Juanatey, Ana Abreu, Enrique Gómez Alvarez, Carlos Ponte-Negretti, Burkhard Weisser, Alexander Parkhomenko, Francisco Araújo, Alvaro Sosa-Liprandi
{"title":"The Polypill (Acetyl Salicylic Acid, Atorvastatin, and Ramipril) Paradigm Shift in Secondary Prevention: Global Expert Delphi Consensus.","authors":"Daniel Piñeiro, José Ramón González-Juanatey, Ana Abreu, Enrique Gómez Alvarez, Carlos Ponte-Negretti, Burkhard Weisser, Alexander Parkhomenko, Francisco Araújo, Alvaro Sosa-Liprandi","doi":"10.5334/gh.1466","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The SECURE trial demonstrated that the cardiovascular (CV)-polypill (acetylsalicylic acid [ASA] + atorvastatin + ramipril) reduces CV mortality by 33% in patients with acute myocardial infarction compared to standard care. The 2023 ACS ESC Guidelines recommend the polypill to improve outcomes and adherence.</p><p><strong>Objective: </strong>This study aims to establish a global consensus on the optimal use of the CV-polypill in secondary prevention.</p><p><strong>Methods: </strong>A two-round, modified Delphi method was used, featuring a 30-statement evidence-based questionnaire validated by eight renowned cardiologists. Fifty clinicians from 19 countries in Europe, Latin America, and Asia were invited to join the Delphi panel. Panelists ranked responses using a three-point Likert scale for agreement and importance. Consensus was defined as ≥80% agreement or rating statements 'very important' or 'important'. Statements without consensus after the first round were refined with evidence and feedback in the second round. Remaining disagreements were resolved in a face-to-face meeting. Descriptive statistics were applied.</p><p><strong>Results: </strong>Response rate was 76% (round 1) and 74% (round 2); 82% were cardiologists, with 74% frequently recommending the CV-polypill. Consensus was achieved on 93.3% of statements. Research showing a 24% relative risk reduction in major adverse CV events over a median of 3 years with the CV-polypill post-acute myocardial infarction, compared to usual care, reached 97.4% agreement for clinical implementation, and a 100% consensus supported polypill use at hospital discharge or first follow-up visits; 81.1% agreed on a prompt initiation after patient stabilization. There was agreement on algorithms for initiating (97.3%), considering patient preferences (97.4%) to the polypill and its cost savings over usual care (89.5%).</p><p><strong>Conclusion: </strong>The Delphi consensus on real-world use of a CV polypill (ASA, atorvastatin, and ramipril) for secondary prevention post-acute coronary syndrome supports early initiation (within 8 days or at discharge). The findings provide a foundation to inform practice and policy, identifying priorities for further research.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"83"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12466114/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1466","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The SECURE trial demonstrated that the cardiovascular (CV)-polypill (acetylsalicylic acid [ASA] + atorvastatin + ramipril) reduces CV mortality by 33% in patients with acute myocardial infarction compared to standard care. The 2023 ACS ESC Guidelines recommend the polypill to improve outcomes and adherence.
Objective: This study aims to establish a global consensus on the optimal use of the CV-polypill in secondary prevention.
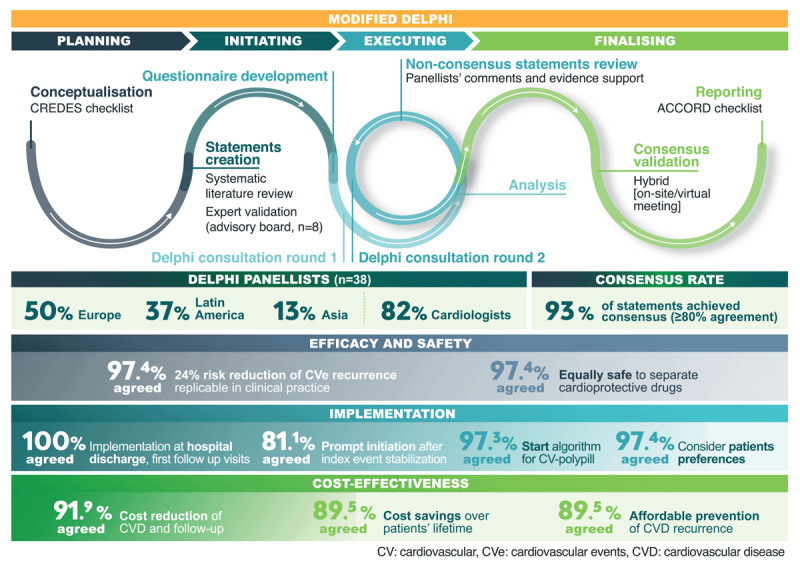
Methods: A two-round, modified Delphi method was used, featuring a 30-statement evidence-based questionnaire validated by eight renowned cardiologists. Fifty clinicians from 19 countries in Europe, Latin America, and Asia were invited to join the Delphi panel. Panelists ranked responses using a three-point Likert scale for agreement and importance. Consensus was defined as ≥80% agreement or rating statements 'very important' or 'important'. Statements without consensus after the first round were refined with evidence and feedback in the second round. Remaining disagreements were resolved in a face-to-face meeting. Descriptive statistics were applied.
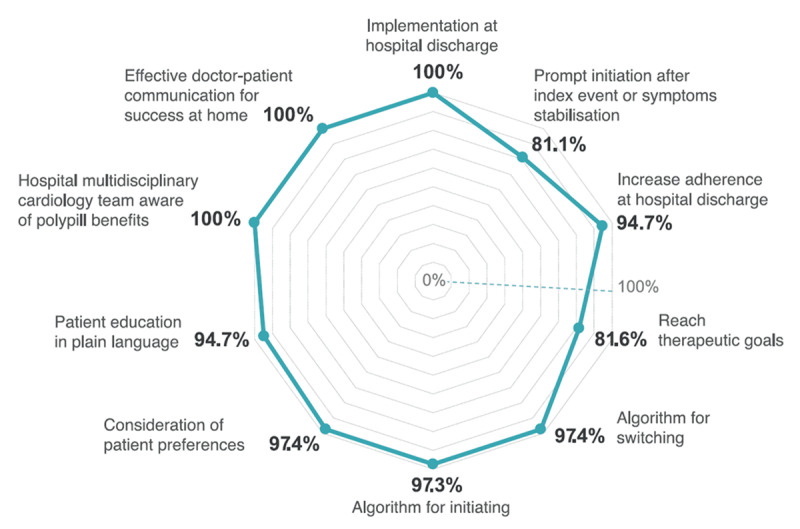
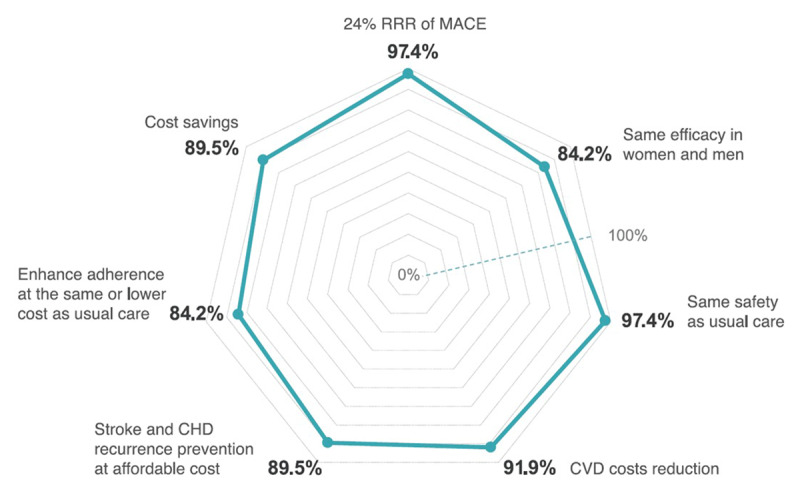
Results: Response rate was 76% (round 1) and 74% (round 2); 82% were cardiologists, with 74% frequently recommending the CV-polypill. Consensus was achieved on 93.3% of statements. Research showing a 24% relative risk reduction in major adverse CV events over a median of 3 years with the CV-polypill post-acute myocardial infarction, compared to usual care, reached 97.4% agreement for clinical implementation, and a 100% consensus supported polypill use at hospital discharge or first follow-up visits; 81.1% agreed on a prompt initiation after patient stabilization. There was agreement on algorithms for initiating (97.3%), considering patient preferences (97.4%) to the polypill and its cost savings over usual care (89.5%).
Conclusion: The Delphi consensus on real-world use of a CV polypill (ASA, atorvastatin, and ramipril) for secondary prevention post-acute coronary syndrome supports early initiation (within 8 days or at discharge). The findings provide a foundation to inform practice and policy, identifying priorities for further research.
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


