Fausto Petrelli, Antonio Ghidini, Maria Chiara Parati, Karen Borgonovo, Mauro Rossitto, Mara Ghilardi, Giuseppina Dognini, Daniela Petro', Irene Angeli, Veronica Lonati, Lorenzo Dottorini, Alessandro Iaculli
{"title":"Immune Checkpoint Inhibitors Beyond Progression in Various Solid Tumors: A Systematic Review and Pooled Analysis.","authors":"Fausto Petrelli, Antonio Ghidini, Maria Chiara Parati, Karen Borgonovo, Mauro Rossitto, Mara Ghilardi, Giuseppina Dognini, Daniela Petro', Irene Angeli, Veronica Lonati, Lorenzo Dottorini, Alessandro Iaculli","doi":"10.3390/jcm14186680","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: Immune checkpoint inhibitors (ICIs) have transformed outcomes in advanced cancers; however, the value of continuing treatment after radiologic progression remains uncertain. We systematically assessed the efficacy and safety of ICI continuation beyond progression, focusing on the objective response rate (ORR), progression-free survival (PFS), and overall survival (OS). <b>Methods:</b> PubMed/MEDLINE, Embase, and the Cochrane Library were searched from inception to 31 March 2025. Eligible reports included retrospective cohorts, prospective trials, post hoc analyses, and pooled regulatory reviews that compared outcomes after ICI continuation versus discontinuation or historical controls. Quality was appraised with the Newcastle-Ottawa Scale (observational designs) and the Cochrane Risk-of-Bias tool (randomized trials). <b>Results:</b> Fifty studies involving 8989 patients met the inclusion criteria: 41 retrospective cohorts; 6 post hoc analyses; 2 randomized trials (1 phase III, 1 phase II); and 1 pooled FDA review. Continuing ICIs beyond progression produced ORRs of 9.3-39% in non-small cell lung cancer (n = 5102), 14-100% in melanoma (n = 669), and 8-33% in renal cell carcinoma (n = 458). Median OS ranged from 8.9 to 18.2 months in lung cancer, 12 to 29.9 months in melanoma, and up to 34.8 months in RCC. Modest but clinically meaningful benefits were reported in colorectal, head-and-neck, gastric, liver, and urothelial tumors. <b>Conclusions:</b> Select patients-particularly those with melanoma, lung cancer, RCC, or gastric cancer-may derive sustained benefit from ICI therapy after radiologic progression. Decisions should incorporate tumor biology, performance status, and emerging biomarkers. Prospective, biomarker-driven trials are needed to define optimal patient selection and the duration of post-progression immunotherapy.</p>","PeriodicalId":15533,"journal":{"name":"Journal of Clinical Medicine","volume":"14 18","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12470277/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcm14186680","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
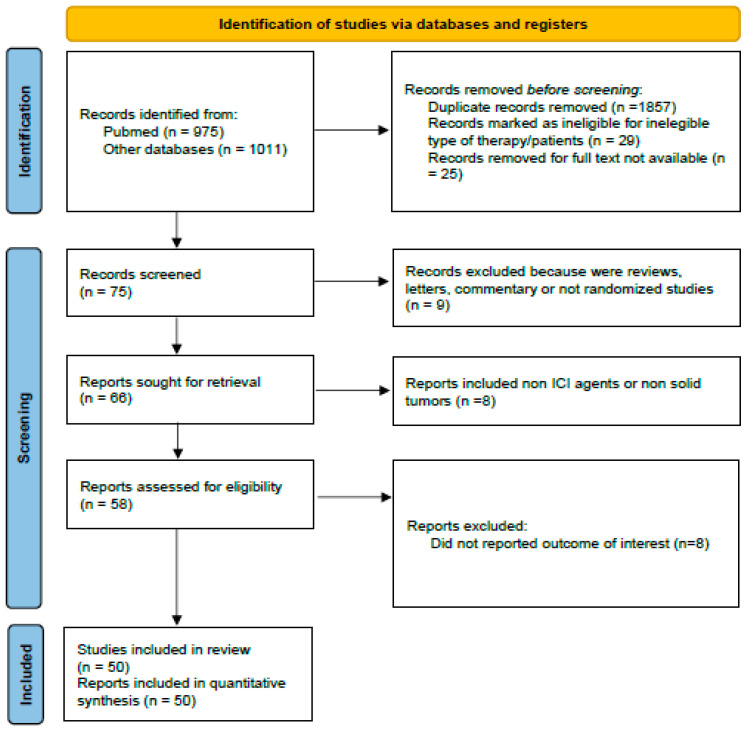
Background: Immune checkpoint inhibitors (ICIs) have transformed outcomes in advanced cancers; however, the value of continuing treatment after radiologic progression remains uncertain. We systematically assessed the efficacy and safety of ICI continuation beyond progression, focusing on the objective response rate (ORR), progression-free survival (PFS), and overall survival (OS). Methods: PubMed/MEDLINE, Embase, and the Cochrane Library were searched from inception to 31 March 2025. Eligible reports included retrospective cohorts, prospective trials, post hoc analyses, and pooled regulatory reviews that compared outcomes after ICI continuation versus discontinuation or historical controls. Quality was appraised with the Newcastle-Ottawa Scale (observational designs) and the Cochrane Risk-of-Bias tool (randomized trials). Results: Fifty studies involving 8989 patients met the inclusion criteria: 41 retrospective cohorts; 6 post hoc analyses; 2 randomized trials (1 phase III, 1 phase II); and 1 pooled FDA review. Continuing ICIs beyond progression produced ORRs of 9.3-39% in non-small cell lung cancer (n = 5102), 14-100% in melanoma (n = 669), and 8-33% in renal cell carcinoma (n = 458). Median OS ranged from 8.9 to 18.2 months in lung cancer, 12 to 29.9 months in melanoma, and up to 34.8 months in RCC. Modest but clinically meaningful benefits were reported in colorectal, head-and-neck, gastric, liver, and urothelial tumors. Conclusions: Select patients-particularly those with melanoma, lung cancer, RCC, or gastric cancer-may derive sustained benefit from ICI therapy after radiologic progression. Decisions should incorporate tumor biology, performance status, and emerging biomarkers. Prospective, biomarker-driven trials are needed to define optimal patient selection and the duration of post-progression immunotherapy.
期刊介绍:
Journal of Clinical Medicine (ISSN 2077-0383), is an international scientific open access journal, providing a platform for advances in health care/clinical practices, the study of direct observation of patients and general medical research. This multi-disciplinary journal is aimed at a wide audience of medical researchers and healthcare professionals.
Unique features of this journal:
manuscripts regarding original research and ideas will be particularly welcomed.JCM also accepts reviews, communications, and short notes.
There is no limit to publication length: our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


