{"title":"Patterns of Prescription Switching in a Uniform-Pricing System for Multi-Source Drugs: A Retrospective Population-Based Cohort Study.","authors":"Dong Han Kim, Song Hee Hong","doi":"10.3390/healthcare13182339","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Generic drugs account for approximately 40% of the Korean prescription drug market, despite limited generic substitution at the point of dispensing. This suggests that switching between originator and generic drugs often occurs at the point of prescription. Physicians, in fact, have opposed pharmacy-level substitution due to concerns about the clinical equivalence of generics, despite the regulatory confirmation of their bioequivalence. Importantly, multi-source prescription switching (MSPS) may reflect discretionary prescribing behavior, underscoring the need for targeted benefit policies to enhance substitutability and promote effective competition among multi-source drugs. This study aimed to quantify the extent of physician-initiated MSPS among adults with hypertension or diabetes and to identify factors associated with these switching behaviors. <b>Methods:</b> We conducted a retrospective cohort study using Korean National Health Insurance claims data. The studied cohort consisted of patients newly initiated, between January and June 2014, on a pharmaceutically equivalent and bioequivalent antihypertensive or antidiabetic drug. Patients were followed for up to 24 months to identify MSPS episodes occurring during drug therapy courses, which were defined as 12 ± 3 consecutive visits resulting in prescriptions for pharmaceutically equivalent, bioequivalent multi-source drugs. An MSPS episode was defined as a change in product code-uniquely identifying a multi-source drug-within the same pharmaceutically equivalent drug code between any two consecutive prescriptions within the course. We estimated the mean MSPS rate and assessed variation by patient characteristics, drug types, physician practices, and geographic regions. <b>Results:</b> Among 1,325,334 identified drug therapy courses, 17.06% involved at least one MSPS. Switching rates varied substantially (coefficient of variation = 227%) by physician practice setting (e.g., public health center branches: 26%; tertiary hospitals: 15%) and by drug market size (e.g., glimepiride: 29%; cilnidipine: 1%). In contrast, patient age and gender were not associated with switching behavior. <b>Conclusions:</b> In Korea, physicians frequently switch prescriptions between originator and generic drugs, even as generic substitution at the pharmacy level remains uncommon. The substantial variation in MSPS across provider settings and drug markets-but not by patient characteristics-underscores the need for targeted pharmacy benefit policies to promote effective substitutability and competition among multi-source drugs.</p>","PeriodicalId":12977,"journal":{"name":"Healthcare","volume":"13 18","pages":""},"PeriodicalIF":2.7000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12469595/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Healthcare","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/healthcare13182339","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
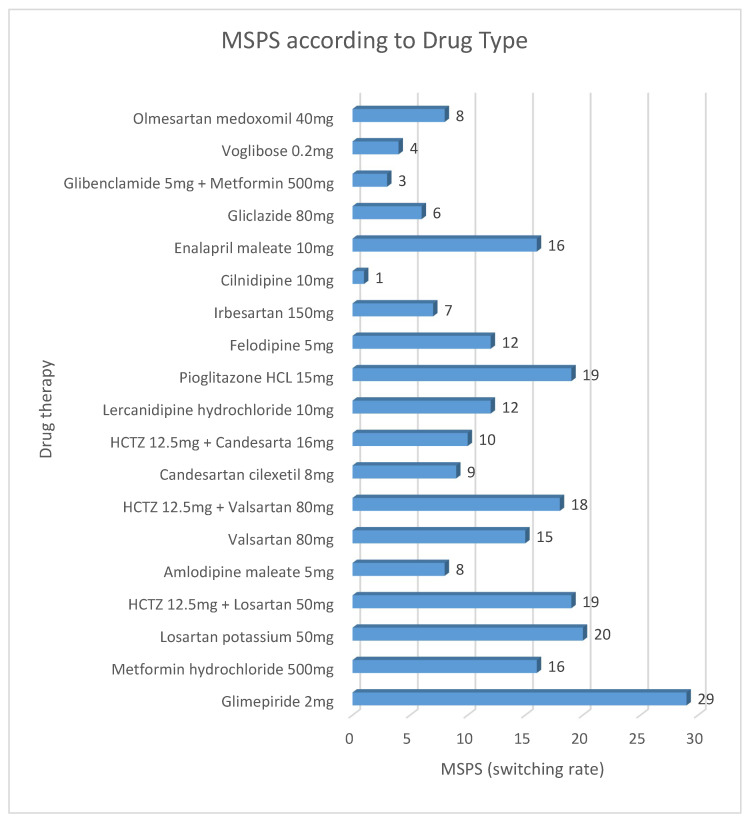
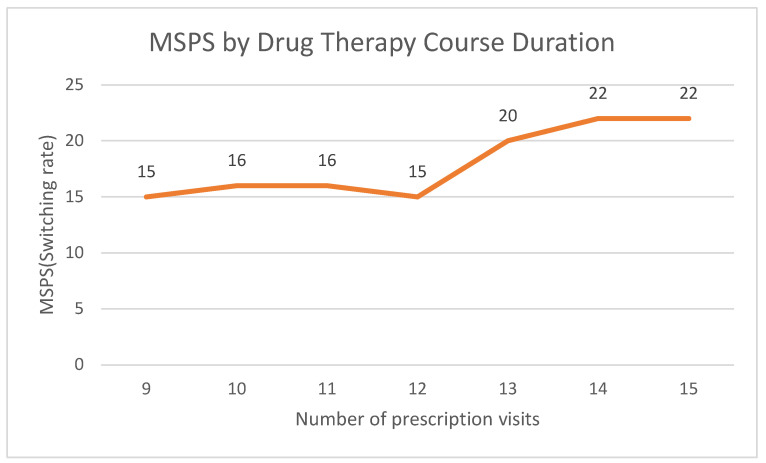
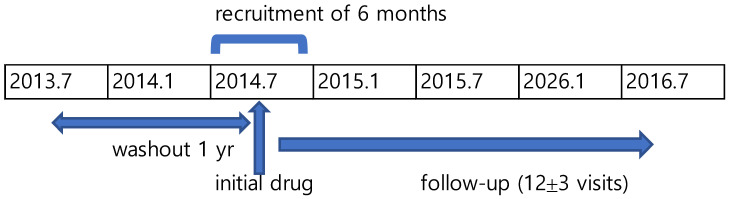
Background: Generic drugs account for approximately 40% of the Korean prescription drug market, despite limited generic substitution at the point of dispensing. This suggests that switching between originator and generic drugs often occurs at the point of prescription. Physicians, in fact, have opposed pharmacy-level substitution due to concerns about the clinical equivalence of generics, despite the regulatory confirmation of their bioequivalence. Importantly, multi-source prescription switching (MSPS) may reflect discretionary prescribing behavior, underscoring the need for targeted benefit policies to enhance substitutability and promote effective competition among multi-source drugs. This study aimed to quantify the extent of physician-initiated MSPS among adults with hypertension or diabetes and to identify factors associated with these switching behaviors. Methods: We conducted a retrospective cohort study using Korean National Health Insurance claims data. The studied cohort consisted of patients newly initiated, between January and June 2014, on a pharmaceutically equivalent and bioequivalent antihypertensive or antidiabetic drug. Patients were followed for up to 24 months to identify MSPS episodes occurring during drug therapy courses, which were defined as 12 ± 3 consecutive visits resulting in prescriptions for pharmaceutically equivalent, bioequivalent multi-source drugs. An MSPS episode was defined as a change in product code-uniquely identifying a multi-source drug-within the same pharmaceutically equivalent drug code between any two consecutive prescriptions within the course. We estimated the mean MSPS rate and assessed variation by patient characteristics, drug types, physician practices, and geographic regions. Results: Among 1,325,334 identified drug therapy courses, 17.06% involved at least one MSPS. Switching rates varied substantially (coefficient of variation = 227%) by physician practice setting (e.g., public health center branches: 26%; tertiary hospitals: 15%) and by drug market size (e.g., glimepiride: 29%; cilnidipine: 1%). In contrast, patient age and gender were not associated with switching behavior. Conclusions: In Korea, physicians frequently switch prescriptions between originator and generic drugs, even as generic substitution at the pharmacy level remains uncommon. The substantial variation in MSPS across provider settings and drug markets-but not by patient characteristics-underscores the need for targeted pharmacy benefit policies to promote effective substitutability and competition among multi-source drugs.
期刊介绍:
Healthcare (ISSN 2227-9032) is an international, peer-reviewed, open access journal (free for readers), which publishes original theoretical and empirical work in the interdisciplinary area of all aspects of medicine and health care research. Healthcare publishes Original Research Articles, Reviews, Case Reports, Research Notes and Short Communications. We encourage researchers to publish their experimental and theoretical results in as much detail as possible. For theoretical papers, full details of proofs must be provided so that the results can be checked; for experimental papers, full experimental details must be provided so that the results can be reproduced. Additionally, electronic files or software regarding the full details of the calculations, experimental procedure, etc., can be deposited along with the publication as “Supplementary Material”.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


