Daniel Jones, Alexander Simone, Caroline Hyun, Caitlin Anstee, Molly Gingrich, James Villeneuve, Daniel French, Brian Johnston, Stephen Gowing, Jonathan Spicer, Lorenzo Ferri, Andrew J E Seely
{"title":"Trends and variations in Canadian thoracic surgical volume and perioperative practice during the COVID-19 pandemic.","authors":"Daniel Jones, Alexander Simone, Caroline Hyun, Caitlin Anstee, Molly Gingrich, James Villeneuve, Daniel French, Brian Johnston, Stephen Gowing, Jonathan Spicer, Lorenzo Ferri, Andrew J E Seely","doi":"10.1503/cjs.001224","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Thoracic surgeons in Canada responded to the COVID-19 pandemic without existing precedence. The primary aim of this study was to understand how thoracic surgery care in Canada was affected by the pandemic in terms of volume, perioperative management, and patterns of practice.</p><p><strong>Methods: </strong>Data were obtained using 2 questionnaires (18-item surgeon-specific and 13-item institution-specific questionnaires) in addition to the Canadian Association of Thoracic Surgery (CATS) national database. Outcomes included qualitative surgeon experiences and thoracic surgery volume from March 2020 to December 2022. Centres were separated into 3 levels of COVID-19 burden based on community prevalence.</p><p><strong>Results: </strong>We received survey responses from 63 surgeons and 6 institutions. In-person consultation dropped by 57% during the pandemic. Preoperative cancer workups experienced minor (≤ 4 wk, 39%) and major (≥ 8 wk, 27%) delays. Operable lung and esophageal cancer experienced minor delays in treatment, while pure ground-glass opacities and benign esophageal pathology experienced major delays (25%) or cancellations (21%). Medical education shifted to virtual platforms, decreasing student involvement by 81%. Perceived factors affecting operating room availability included lack of staff, beds, and personal protective equipment.</p><p><strong>Conclusion: </strong>There was a pan-Canadian reduction in thoracic surgery volume, regardless of regional COVID-19 caseload. Prioritization of thoracic oncology was observed, with a delay in care for minimally invasive and benign illness. Our findings illustrate how surgeons and institutions responded to the pandemic and inform strategies for Canadian thoracic practice in the event of future analogous events.</p>","PeriodicalId":9573,"journal":{"name":"Canadian Journal of Surgery","volume":"68 5","pages":"E365-E375"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12479119/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cjs.001224","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Thoracic surgeons in Canada responded to the COVID-19 pandemic without existing precedence. The primary aim of this study was to understand how thoracic surgery care in Canada was affected by the pandemic in terms of volume, perioperative management, and patterns of practice.
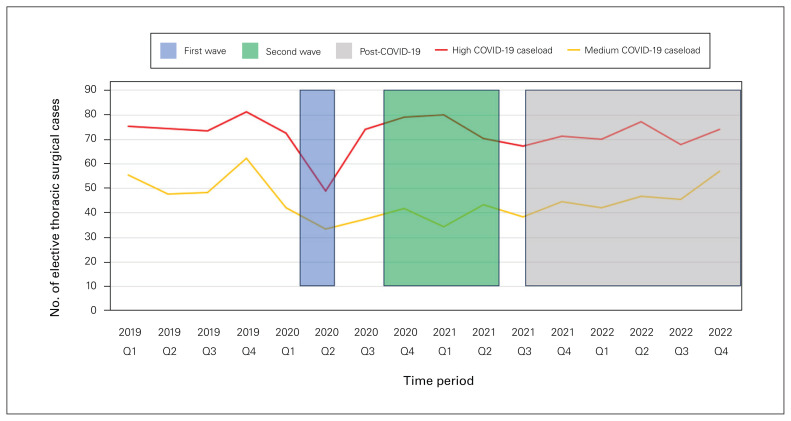
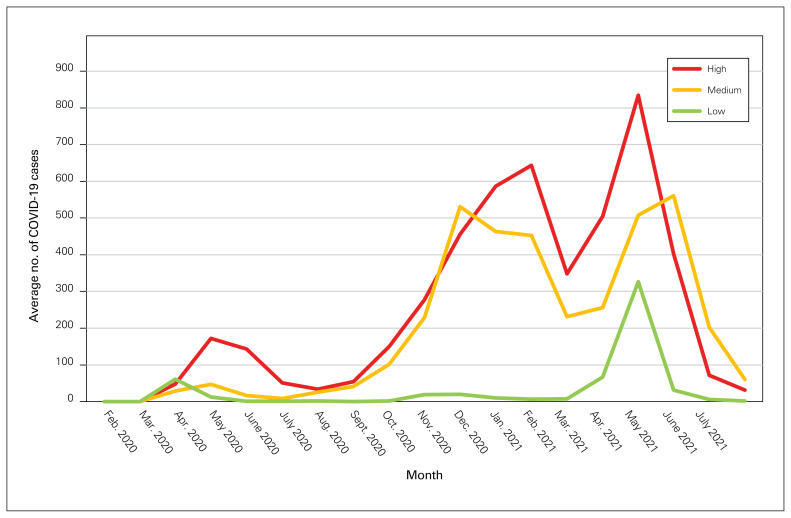
Methods: Data were obtained using 2 questionnaires (18-item surgeon-specific and 13-item institution-specific questionnaires) in addition to the Canadian Association of Thoracic Surgery (CATS) national database. Outcomes included qualitative surgeon experiences and thoracic surgery volume from March 2020 to December 2022. Centres were separated into 3 levels of COVID-19 burden based on community prevalence.
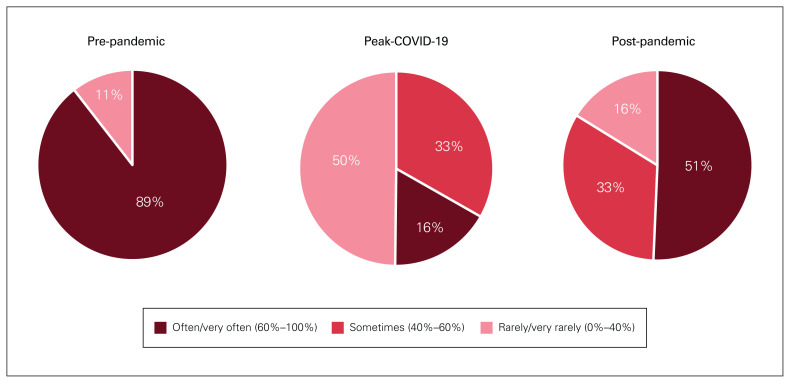
Results: We received survey responses from 63 surgeons and 6 institutions. In-person consultation dropped by 57% during the pandemic. Preoperative cancer workups experienced minor (≤ 4 wk, 39%) and major (≥ 8 wk, 27%) delays. Operable lung and esophageal cancer experienced minor delays in treatment, while pure ground-glass opacities and benign esophageal pathology experienced major delays (25%) or cancellations (21%). Medical education shifted to virtual platforms, decreasing student involvement by 81%. Perceived factors affecting operating room availability included lack of staff, beds, and personal protective equipment.
Conclusion: There was a pan-Canadian reduction in thoracic surgery volume, regardless of regional COVID-19 caseload. Prioritization of thoracic oncology was observed, with a delay in care for minimally invasive and benign illness. Our findings illustrate how surgeons and institutions responded to the pandemic and inform strategies for Canadian thoracic practice in the event of future analogous events.
期刊介绍:
The mission of CJS is to contribute to the meaningful continuing medical education of Canadian surgical specialists, and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical and basic science research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


