Impact of Sacubitril/Valsartan (ARNI) Compared with ACEI/ARB in Patients with Acute Myocardial Infarction on Post-Infarction Left Ventricular Systolic Dysfunction: A Retrospective Analysis.
Rafał Niemiec, Małgorzata Niemiec, Martyna Nowak, Barbara Gurba, Monika Bujak, Katarzyna Chowaniec-Rybka, Magdalena Sowier, Agnieszka Nowotarska, Bartosz Gruchlik, Adam Pytlewski, Katarzyna Mizia-Stec
{"title":"Impact of Sacubitril/Valsartan (ARNI) Compared with ACEI/ARB in Patients with Acute Myocardial Infarction on Post-Infarction Left Ventricular Systolic Dysfunction: A Retrospective Analysis.","authors":"Rafał Niemiec, Małgorzata Niemiec, Martyna Nowak, Barbara Gurba, Monika Bujak, Katarzyna Chowaniec-Rybka, Magdalena Sowier, Agnieszka Nowotarska, Bartosz Gruchlik, Adam Pytlewski, Katarzyna Mizia-Stec","doi":"10.3390/biomedicines13092265","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objectives</b>: Angiotensin receptor-neprilysin inhibitor (ARNI) has a well-established advantage over angiotensin-converting enzyme inhibitor or angiotensin receptor blocker (ACEI/ARB) therapy in patients (pts) with heart failure with reduced ejection fraction (HFrEF), but in pts after acute myocardial infarction (AMI) with left ventricular (LV) systolic dysfunction, the advantage of ARNI has not been clearly proven. The efficacy of ARNI is compared with that of ACEI/ARB therapy in patients with their first AMI in terms of improvement of post-infarction LV systolic function. <b>Methods</b>: The study was conducted as a retrospective one-center cross-sectional analysis. Overall, 1473 pts (990 M, median age 71 [64; 77]) with AMI (their first AMI, complete coronary revascularization, no prior coronary revascularization or history of HF) hospitalized in 2022-2024 were enrolled in a retrospective cross-sectional analysis. The study population was categorized into pts receiving ARNI and ACEI/ARB. Then, based on the ARNI subgroup, matching that included age, sex, and LV ejection fraction (LVEF) was performed by using the 1:1 nearest neighbor method without returning. Finally, two groups (ARNI vs. ACEI/ARB) of 30 pts were obtained and analyzed at baseline and at a 6-week follow-up. The improvement of post-infarction LV systolic function was obtained in terms of LVEF, ΔLVEF, and relative ΔLVEF values (ΔLVEF/baseline LVEF). <b>Results</b>: The comparison of baseline characteristics revealed borderline lower initial LVEF (30 vs. 36%, <i>p</i> = 0.076) and a higher frequency of SGLT-2 inhibitor use (70% vs. 36.7%, <i>p</i> = 0.01) in the ARNI subgroup. At the 6-week follow-up, in both subgroups, a significant improvement in the median LVEF values was achieved-from a median LVEF value of 30% (27.3; 38) to 37% (30; 43; <i>p</i> = 0.0008) in the ARNI subgroup and from a median LVEF value of 36% (33; 39) to 45% (42; 52; <i>p</i> < 0.0001) in the ACEI/ARB subgroup. The median ΔLVEF in the ACEI/ARB subgroup was higher [10% (6; 12)] than in the ARNI subgroup [6% (2; 10.25), <i>p</i> = 0.018]. Similarly, the median relative ΔLVEF was higher in the ACEI/ARB subgroup [30% (15.4; 40)] than in the ARNI group [17.5% (7; 31.9), <i>p</i> = 0.047]. The vast majority of patients, particularly in the ARNI group (99.7%), were treated with the lowest available dose of the drug. <b>Conclusions</b>: Our current experience in ARNI therapy after AMI is promising; however, it is limited to a small group of patients with severe impairment of LV systolic function. Regardless of the significant improvement in the baseline LVEF observed in patients receiving both ACEI/ARB and ARNI at the 6-week follow-up, the absolute and relative increases in the LVEF were higher in subjects treated with ACEI/ARB. However, the clinical benefits of ARNI therapy may emerge more gradually, and its advantages could become more apparent over a longer follow-up period. The clinical efficacy of early use of ARNI in the setting of AMI needs further evaluation.</p>","PeriodicalId":8937,"journal":{"name":"Biomedicines","volume":"13 9","pages":""},"PeriodicalIF":3.9000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12467660/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedicines","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.3390/biomedicines13092265","RegionNum":3,"RegionCategory":"工程技术","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
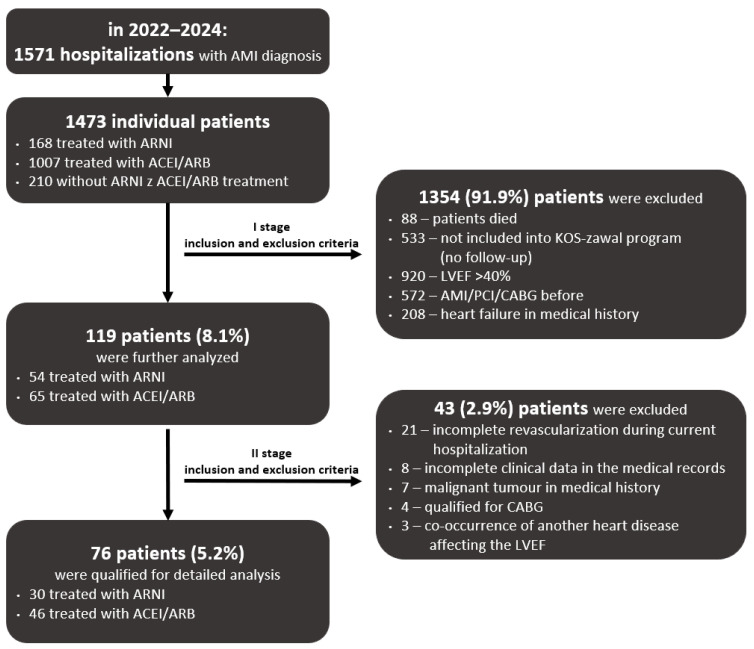
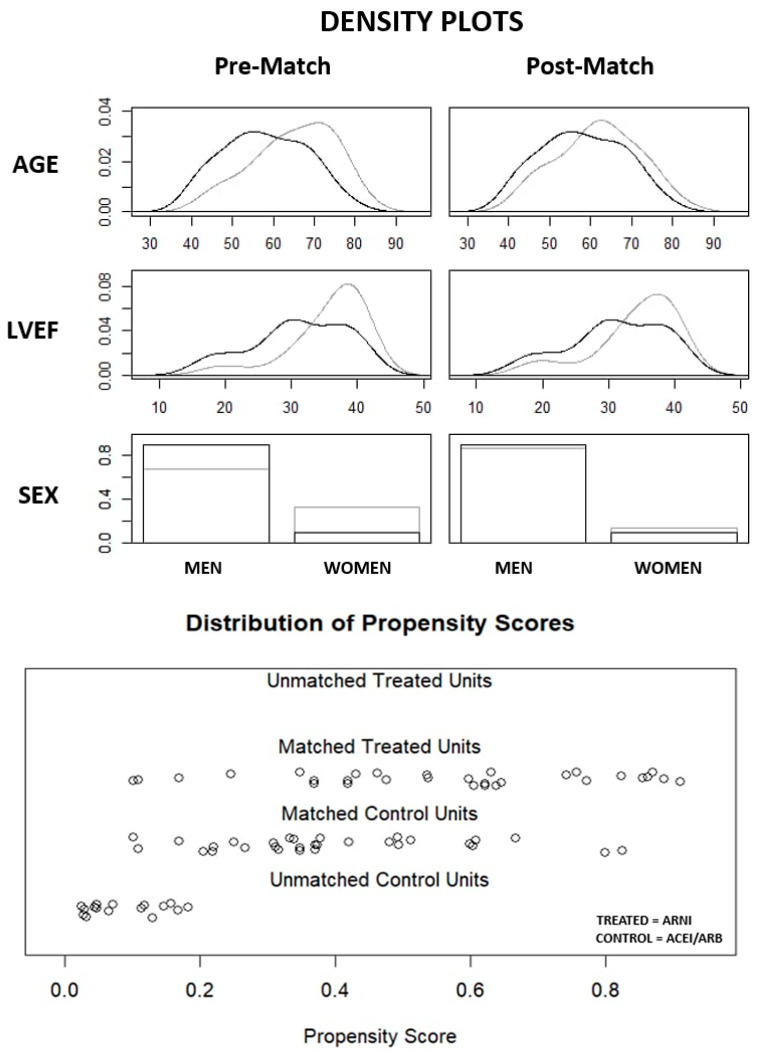
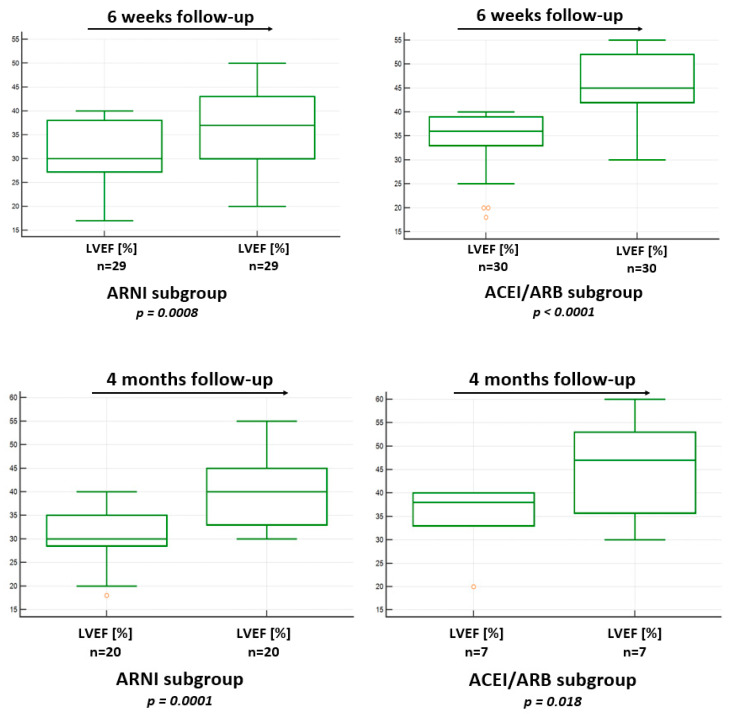
Background/Objectives: Angiotensin receptor-neprilysin inhibitor (ARNI) has a well-established advantage over angiotensin-converting enzyme inhibitor or angiotensin receptor blocker (ACEI/ARB) therapy in patients (pts) with heart failure with reduced ejection fraction (HFrEF), but in pts after acute myocardial infarction (AMI) with left ventricular (LV) systolic dysfunction, the advantage of ARNI has not been clearly proven. The efficacy of ARNI is compared with that of ACEI/ARB therapy in patients with their first AMI in terms of improvement of post-infarction LV systolic function. Methods: The study was conducted as a retrospective one-center cross-sectional analysis. Overall, 1473 pts (990 M, median age 71 [64; 77]) with AMI (their first AMI, complete coronary revascularization, no prior coronary revascularization or history of HF) hospitalized in 2022-2024 were enrolled in a retrospective cross-sectional analysis. The study population was categorized into pts receiving ARNI and ACEI/ARB. Then, based on the ARNI subgroup, matching that included age, sex, and LV ejection fraction (LVEF) was performed by using the 1:1 nearest neighbor method without returning. Finally, two groups (ARNI vs. ACEI/ARB) of 30 pts were obtained and analyzed at baseline and at a 6-week follow-up. The improvement of post-infarction LV systolic function was obtained in terms of LVEF, ΔLVEF, and relative ΔLVEF values (ΔLVEF/baseline LVEF). Results: The comparison of baseline characteristics revealed borderline lower initial LVEF (30 vs. 36%, p = 0.076) and a higher frequency of SGLT-2 inhibitor use (70% vs. 36.7%, p = 0.01) in the ARNI subgroup. At the 6-week follow-up, in both subgroups, a significant improvement in the median LVEF values was achieved-from a median LVEF value of 30% (27.3; 38) to 37% (30; 43; p = 0.0008) in the ARNI subgroup and from a median LVEF value of 36% (33; 39) to 45% (42; 52; p < 0.0001) in the ACEI/ARB subgroup. The median ΔLVEF in the ACEI/ARB subgroup was higher [10% (6; 12)] than in the ARNI subgroup [6% (2; 10.25), p = 0.018]. Similarly, the median relative ΔLVEF was higher in the ACEI/ARB subgroup [30% (15.4; 40)] than in the ARNI group [17.5% (7; 31.9), p = 0.047]. The vast majority of patients, particularly in the ARNI group (99.7%), were treated with the lowest available dose of the drug. Conclusions: Our current experience in ARNI therapy after AMI is promising; however, it is limited to a small group of patients with severe impairment of LV systolic function. Regardless of the significant improvement in the baseline LVEF observed in patients receiving both ACEI/ARB and ARNI at the 6-week follow-up, the absolute and relative increases in the LVEF were higher in subjects treated with ACEI/ARB. However, the clinical benefits of ARNI therapy may emerge more gradually, and its advantages could become more apparent over a longer follow-up period. The clinical efficacy of early use of ARNI in the setting of AMI needs further evaluation.
BiomedicinesBiochemistry, Genetics and Molecular Biology-General Biochemistry,Genetics and Molecular Biology
CiteScore
5.20
自引率
8.50%
发文量
2823
审稿时长
8 weeks
期刊介绍:
Biomedicines (ISSN 2227-9059; CODEN: BIOMID) is an international, scientific, open access journal on biomedicines published quarterly online by MDPI.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


