Sujin Kim, Andrew J Whipkey, Jihye Bae, Avinash Bhakta
{"title":"Digital health interventions for colorectal cancer screening uptake: A scoping review.","authors":"Sujin Kim, Andrew J Whipkey, Jihye Bae, Avinash Bhakta","doi":"10.1371/journal.pdig.0001028","DOIUrl":null,"url":null,"abstract":"<p><p>Digital health interventions (DHIs) are increasingly employed to improve colorectal cancer (CRC) screening uptake, yet comprehensive syntheses of their effectiveness across diverse contexts remain scarce. This scoping review examines how individual, contextual, technological, and timing-related factors shape CRC screening outcomes in DHI-based trials. Following PRISMA-ScR guidelines, we conducted a systematic search of PubMed, Google Scholar, and ClinicalTrials.gov from March 1 to April 20, 2024, identifying 4,523 records through databases and an additional 2,039 through backward citation tracking. After deduplication and screening, 51 studies were included and charted using the PICOT (Population, Intervention, Comparison, Outcome, and Timing) framework. Included studies spanned urban health systems, rural community clinics, and Federally Qualified Health Centers in the United States, Europe, Asia, and Australia, with intervention durations ranging from six weeks to ten years. Keyword co-occurrence mapping revealed four thematic domains: (1) patient-centered technology and adherence, (2) behavioral design and personalization, (3) clinical workflow and provider interaction, and (4) equity, disparities, and community engagement. Findings showed that tailored telephone outreach, mailed fecal immunochemical testing combined with navigation support, EMR-based automated reminders, and mobile applications delivering personalized education increased screening rates by 20.9% to 37.7% compared with conventional approaches. Hybrid models combining digital tools with human facilitation were particularly effective for underserved populations, including racial and ethnic minorities, rural communities, and individuals with limited health literacy. However, research gaps persist for younger adults at risk for early-onset CRC and for understanding the long-term sustainability and cost-effectiveness of digital interventions. Temporal aspects such as intervention timing, frequency, and duration were identified as important factors but were inconsistently reported. Future research should address digital health literacy, implementation barriers, and long-term follow-up to support sustained CRC screening adherence through user-centered, scalable, and culturally responsive digital solutions.</p>","PeriodicalId":74465,"journal":{"name":"PLOS digital health","volume":"4 9","pages":"e0001028"},"PeriodicalIF":7.7000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12463253/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLOS digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pdig.0001028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
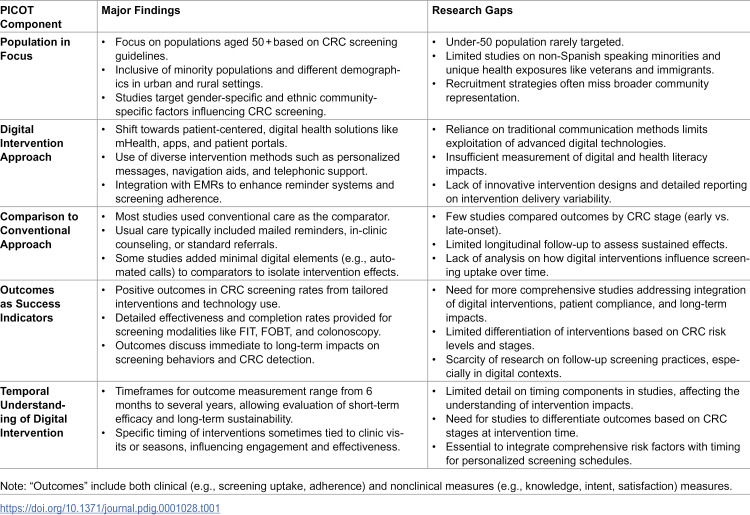
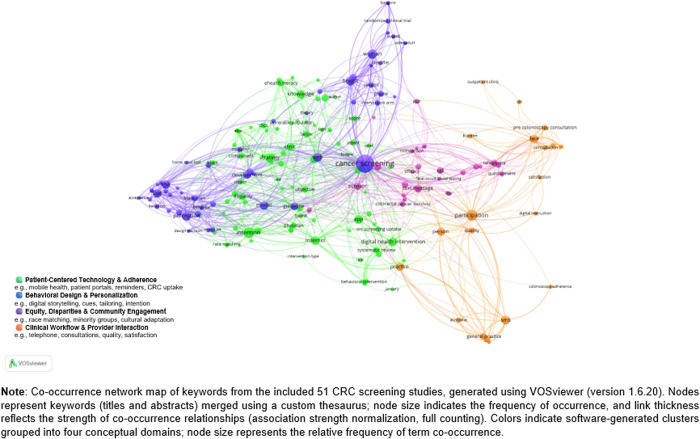
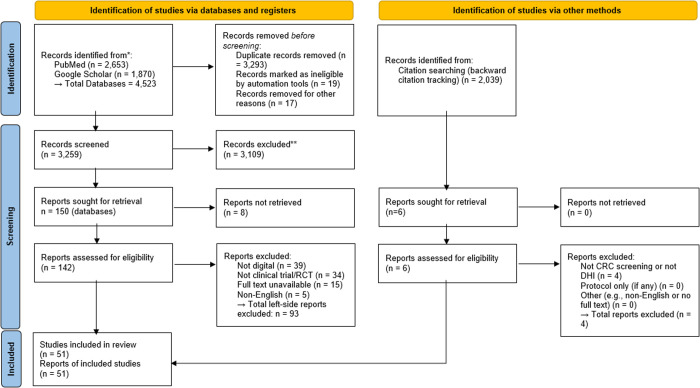
Digital health interventions (DHIs) are increasingly employed to improve colorectal cancer (CRC) screening uptake, yet comprehensive syntheses of their effectiveness across diverse contexts remain scarce. This scoping review examines how individual, contextual, technological, and timing-related factors shape CRC screening outcomes in DHI-based trials. Following PRISMA-ScR guidelines, we conducted a systematic search of PubMed, Google Scholar, and ClinicalTrials.gov from March 1 to April 20, 2024, identifying 4,523 records through databases and an additional 2,039 through backward citation tracking. After deduplication and screening, 51 studies were included and charted using the PICOT (Population, Intervention, Comparison, Outcome, and Timing) framework. Included studies spanned urban health systems, rural community clinics, and Federally Qualified Health Centers in the United States, Europe, Asia, and Australia, with intervention durations ranging from six weeks to ten years. Keyword co-occurrence mapping revealed four thematic domains: (1) patient-centered technology and adherence, (2) behavioral design and personalization, (3) clinical workflow and provider interaction, and (4) equity, disparities, and community engagement. Findings showed that tailored telephone outreach, mailed fecal immunochemical testing combined with navigation support, EMR-based automated reminders, and mobile applications delivering personalized education increased screening rates by 20.9% to 37.7% compared with conventional approaches. Hybrid models combining digital tools with human facilitation were particularly effective for underserved populations, including racial and ethnic minorities, rural communities, and individuals with limited health literacy. However, research gaps persist for younger adults at risk for early-onset CRC and for understanding the long-term sustainability and cost-effectiveness of digital interventions. Temporal aspects such as intervention timing, frequency, and duration were identified as important factors but were inconsistently reported. Future research should address digital health literacy, implementation barriers, and long-term follow-up to support sustained CRC screening adherence through user-centered, scalable, and culturally responsive digital solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


