{"title":"Novel Computed Tomography Perfusion and Laboratory Indices as Predictors of Long-Term Outcome and Survival in Acute Ischemic Stroke.","authors":"Eray Halil, Kostadin Kostadinov, Nikoleta Traykova, Neli Atanasova, Kiril Atliev, Elizabet Dzhambazova, Penka Atanassova","doi":"10.3390/neurolint17090136","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>Acute ischemic stroke is a leading cause of mortality and long-term disability globally, with limited reliable early predictors of functional outcomes and survival. This study aimed to assess the prognostic value of two novel predictors: the hypoperfusion intensity ratio calculated from mean transit time and time-to-drain maps (HIR-MTT-TTD), derived from computed tomography perfusion (CTP) imaging parameters, and the Inflammation-Coagulation Index (ICI), which integrates systemic inflammatory (C-reactive protein and white blood cell count) and hemostatic (D-dimer) markers.</p><p><strong>Methods: </strong>This prospective, single-center observational study included 60 patients with acute ischemic stroke treated with intravenous thrombolysis and underwent pre-treatment CTP imaging. HIR-MTT-TTD evaluated collateral status and perfusion deficit severity, while ICI integrated C-reactive protein (CRP), white blood cell (WBC) count, and D-dimer levels. Functional outcomes were assessed using the National Institutes of Health Stroke Scale (NIHSS), Barthel Index, and modified Rankin Scale (mRS) at 24 h, 3 months, and 1 year.</p><p><strong>Results: </strong>Of 60 patients, 53.3% achieved functional independence (mRS 0-2) at 1 year. Unadjusted Cox models showed HIR-MTT-TTD (HR = 6.25, 95% CI: 1.48-26.30, <i>p</i> = 0.013) and ICI (HR = 1.08, 95% CI: 1.00-1.17, <i>p</i> = 0.052) were associated with higher 12-month mortality, worse mRS, and lower Barthel scores. After adjustment for age, BMI, smoking status, and sex, these associations became non-significant (HIR-MTT-TTD: HR = 2.83, 95% CI: 0.37-21.37, <i>p</i> = 0.314; ICI: HR = 1.07, 95% CI: 0.96-1.19, <i>p</i> = 0.211). Receiver operating characteristic (ROC) analysis indicated moderate predictive value, with ICI (AUC = 0.756, 95% CI: 0.600-0.867) outperforming HIR-MTT-TTD (AUC = 0.67, 95% CI: 0.48-0.83) for mortality prediction.</p><p><strong>Conclusions: </strong>The study introduces promising prognostic tools for functional outcomes. Elevated HIR-MTT-TTD and ICI values were independently associated with greater initial stroke severity, poorer functional recovery, and increased 1-year mortality. These findings underscore the prognostic significance of hypoperfusion intensity and systemic thrombo-inflammation in acute ischemic stroke. Combining the use of the presented indices may enhance early risk stratification and guide individualized treatment strategies.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"17 9","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12472316/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint17090136","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background/objectives: Acute ischemic stroke is a leading cause of mortality and long-term disability globally, with limited reliable early predictors of functional outcomes and survival. This study aimed to assess the prognostic value of two novel predictors: the hypoperfusion intensity ratio calculated from mean transit time and time-to-drain maps (HIR-MTT-TTD), derived from computed tomography perfusion (CTP) imaging parameters, and the Inflammation-Coagulation Index (ICI), which integrates systemic inflammatory (C-reactive protein and white blood cell count) and hemostatic (D-dimer) markers.
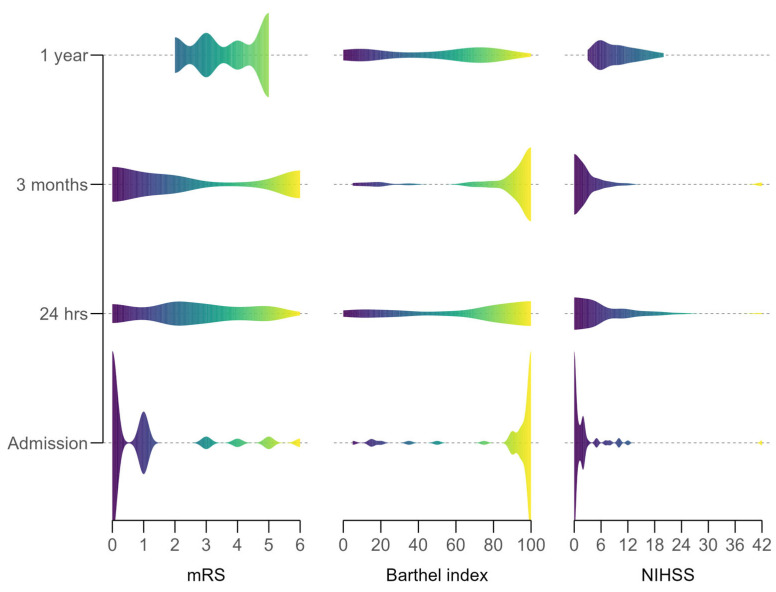
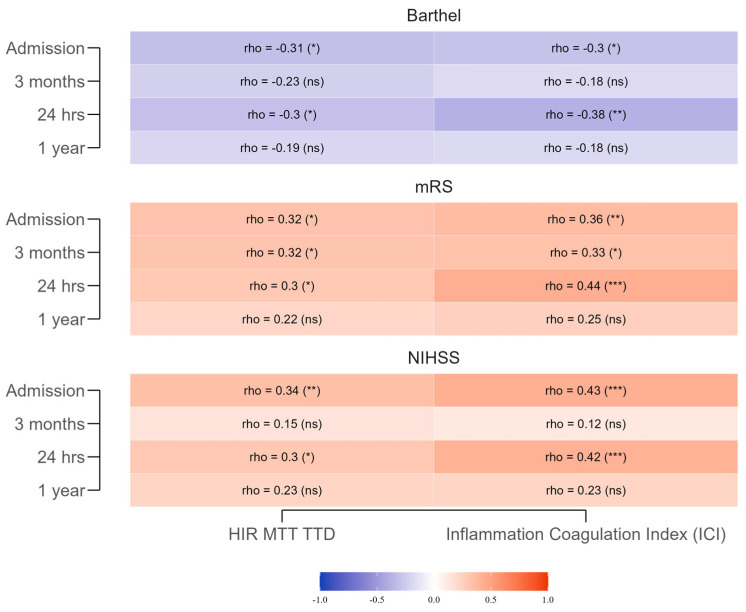
Methods: This prospective, single-center observational study included 60 patients with acute ischemic stroke treated with intravenous thrombolysis and underwent pre-treatment CTP imaging. HIR-MTT-TTD evaluated collateral status and perfusion deficit severity, while ICI integrated C-reactive protein (CRP), white blood cell (WBC) count, and D-dimer levels. Functional outcomes were assessed using the National Institutes of Health Stroke Scale (NIHSS), Barthel Index, and modified Rankin Scale (mRS) at 24 h, 3 months, and 1 year.
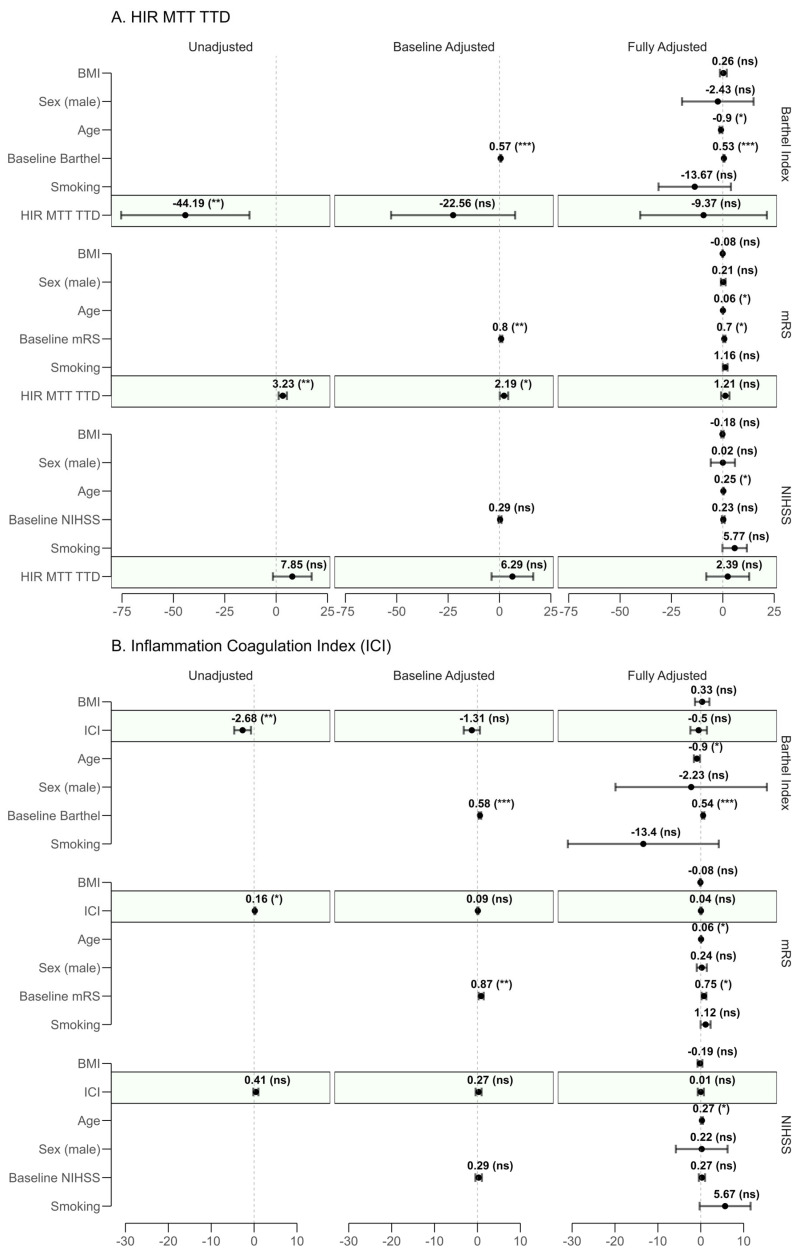
Results: Of 60 patients, 53.3% achieved functional independence (mRS 0-2) at 1 year. Unadjusted Cox models showed HIR-MTT-TTD (HR = 6.25, 95% CI: 1.48-26.30, p = 0.013) and ICI (HR = 1.08, 95% CI: 1.00-1.17, p = 0.052) were associated with higher 12-month mortality, worse mRS, and lower Barthel scores. After adjustment for age, BMI, smoking status, and sex, these associations became non-significant (HIR-MTT-TTD: HR = 2.83, 95% CI: 0.37-21.37, p = 0.314; ICI: HR = 1.07, 95% CI: 0.96-1.19, p = 0.211). Receiver operating characteristic (ROC) analysis indicated moderate predictive value, with ICI (AUC = 0.756, 95% CI: 0.600-0.867) outperforming HIR-MTT-TTD (AUC = 0.67, 95% CI: 0.48-0.83) for mortality prediction.
Conclusions: The study introduces promising prognostic tools for functional outcomes. Elevated HIR-MTT-TTD and ICI values were independently associated with greater initial stroke severity, poorer functional recovery, and increased 1-year mortality. These findings underscore the prognostic significance of hypoperfusion intensity and systemic thrombo-inflammation in acute ischemic stroke. Combining the use of the presented indices may enhance early risk stratification and guide individualized treatment strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


