Julien Dessajan, Aude Gibelin, Matthias Barral, Nina de Montmollin, Vincent Labbé, Michel Djibré, Guillaume Voiriot, Matthieu Turpin, Antoine Parrot, Muriel Fartoukh
{"title":"Severe hemoptysis: etiologies, management, and outcomes from a single-center experience over the last decade.","authors":"Julien Dessajan, Aude Gibelin, Matthias Barral, Nina de Montmollin, Vincent Labbé, Michel Djibré, Guillaume Voiriot, Matthieu Turpin, Antoine Parrot, Muriel Fartoukh","doi":"10.1186/s13613-025-01558-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Data on severe hemoptysis (SH) in the intensive care unit (ICU) remain scarce. We aimed to describe its clinical characteristics, etiologies, management strategies, and outcomes. This retrospective observational study analyzed patients admitted for SH to a referral center between 2009 and 2019. Data were compared to a historical cohort (1995-2009) using the Cochran-Armitage test.</p><p><strong>Results: </strong>A total of 945 patients (75% males; median age 55 years [IQR 42-65]) were analyzed; 67% had respiratory comorbidities. Invasive mechanical ventilation was required in 13% within 24 h of ICU admission. Lung cancer was the leading cause of SH, followed by bronchiectasis, tuberculosis, pneumonia, and aspergillosis. Compared with the historical cohort, pneumonia-related hemoptysis increased (11% vs. 5%; P < 0·001), as did pulmonary arterial involvement (12% vs. 5%; P < 0·001), mainly associated with pneumonia (23%), cancer, or aspergillosis (each 20%). Vascular interventional radiology (VIR) was first attempted in 81% of cases, achieving bleeding control in more than 90% of cases. Major adverse events occurred in 4.4% of cases. Emergent surgical lung resection (within 72 h) was performed in 2% of cases, all after VIR. In-hospital mortality rate increased slightly (8.7% vs. 6.5%; P = 0.08).</p><p><strong>Conclusions: </strong>Over the past decade, lung cancer became the leading cause of SH, with pneumonia increasingly contributing to pulmonary arterial involvement, reinforcing the need for multi-detector computed tomography angiography (MDCTA) screening. The high success rate of VIR confirms its key role, while surgery remains limited to rare cases. In-hospital mortality slightly increased, driven by a higher proportion of lung cancer.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"137"},"PeriodicalIF":5.5000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12463777/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01558-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
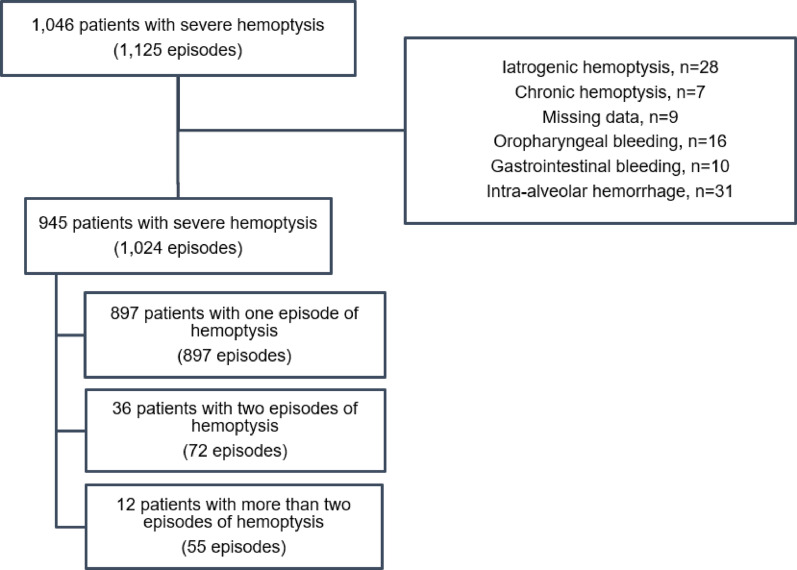
Background: Data on severe hemoptysis (SH) in the intensive care unit (ICU) remain scarce. We aimed to describe its clinical characteristics, etiologies, management strategies, and outcomes. This retrospective observational study analyzed patients admitted for SH to a referral center between 2009 and 2019. Data were compared to a historical cohort (1995-2009) using the Cochran-Armitage test.
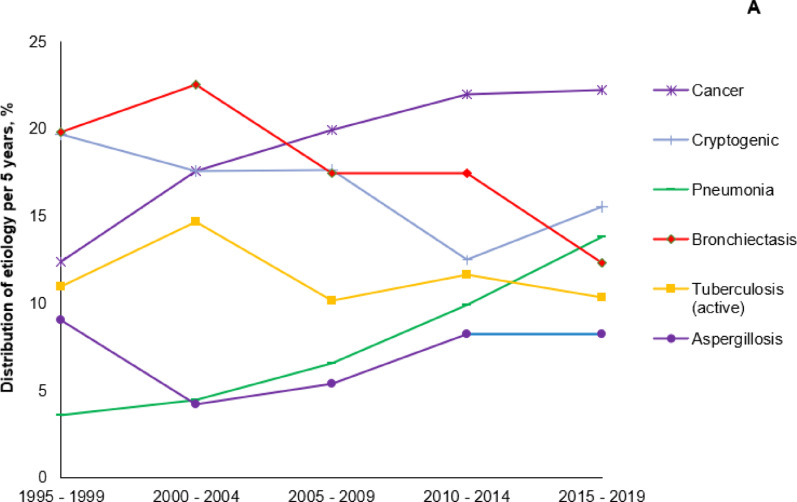
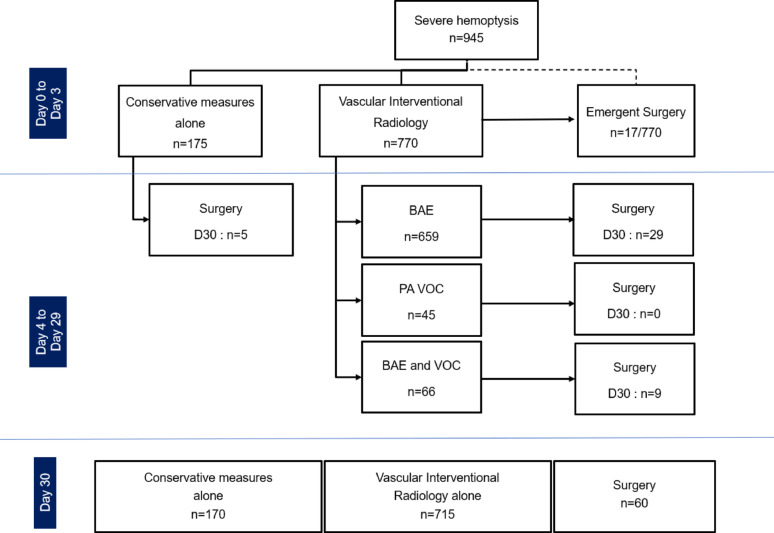
Results: A total of 945 patients (75% males; median age 55 years [IQR 42-65]) were analyzed; 67% had respiratory comorbidities. Invasive mechanical ventilation was required in 13% within 24 h of ICU admission. Lung cancer was the leading cause of SH, followed by bronchiectasis, tuberculosis, pneumonia, and aspergillosis. Compared with the historical cohort, pneumonia-related hemoptysis increased (11% vs. 5%; P < 0·001), as did pulmonary arterial involvement (12% vs. 5%; P < 0·001), mainly associated with pneumonia (23%), cancer, or aspergillosis (each 20%). Vascular interventional radiology (VIR) was first attempted in 81% of cases, achieving bleeding control in more than 90% of cases. Major adverse events occurred in 4.4% of cases. Emergent surgical lung resection (within 72 h) was performed in 2% of cases, all after VIR. In-hospital mortality rate increased slightly (8.7% vs. 6.5%; P = 0.08).
Conclusions: Over the past decade, lung cancer became the leading cause of SH, with pneumonia increasingly contributing to pulmonary arterial involvement, reinforcing the need for multi-detector computed tomography angiography (MDCTA) screening. The high success rate of VIR confirms its key role, while surgery remains limited to rare cases. In-hospital mortality slightly increased, driven by a higher proportion of lung cancer.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


