Sepsis-induced myocardial dysfunction diagnosed with strain versus non-strain echocardiography parameters: incidence, evolution and association with prognosis.
Filipe André Gonzalez, Jacobo Bacariza, Ana Rita Varudo, João Leote, Ricardo Meireles Mateus, Cristina Maia Martins, Maria Inês Ribeiro, Filippo Sanfilippo, Luís Rocha Lopes, Ana G Almeida
{"title":"Sepsis-induced myocardial dysfunction diagnosed with strain versus non-strain echocardiography parameters: incidence, evolution and association with prognosis.","authors":"Filipe André Gonzalez, Jacobo Bacariza, Ana Rita Varudo, João Leote, Ricardo Meireles Mateus, Cristina Maia Martins, Maria Inês Ribeiro, Filippo Sanfilippo, Luís Rocha Lopes, Ana G Almeida","doi":"10.1186/s13613-025-01561-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis-induced myocardial dysfunction (SIMD) remains poorly defined due to scarce longitudinal studies with advanced echocardiography. We characterized SIMD progression using speckle tracking echocardiography (STE).</p><p><strong>Methods: </strong>Prospective single-center study in septic shock patients admitted to intensive care. SIMD was defined as any left ventricular (LV, systolic and/or diastolic) and/or right ventricular (RV) systolic dysfunction, using STE or non-STE criteria, on days 1, 7 and 30. We studied prevalence, evolution and prognosis of SIMD classified with either criteria using Cox regression.</p><p><strong>Results: </strong>Ninety-eight consecutive patients were included. On day 1, SIMD was identified in n = 57/98 (58.2%) and n = 70/98 (71.4%;p = 0.072) by non-STE and STE parameters, respectively. No significant difference in diagnosis was seen for LV diastolic dysfunction: n = 50/98 (51.0%, non-STE) vs. n = 51/98 (52.0%, STE; p = 1.00). Prevalences of LV and RV systolic dysfunction were not significantly higher with STE criteria: n = 59/98 (60.2%, STE) vs. n = 47/98 (48.0%, non-STE; p = 0.115) for LV; n = 39/98 (39.8%, STE) vs. n = 27/98 (27.6%, non-STE; p = 0.096) for RV. More patients recovered from SIMD when evaluated with non-STE criteria at day 7 (35.3% vs. 17.5% STE; p = 0.033), but not at day 30 (24.5% vs. 18.8% STE; p = 0.501). The 30-day mortality (n = 33/98, 33.7%) was associated with SIMD diagnosed using non-STE (p = 0.010), but not with STE (p = 0.057). In Cox regression, only LVDD by non-STE criteria predicted 30-day mortality (p = 0.005).</p><p><strong>Conclusions: </strong>The incidence of SIMD in septic shock is higher when using STE criteria, with lower reversibility in the first week. A broad definition of SIMD utilizing STE criteria does not seem to provide additional prognostic value.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov: NCT05552521 registered on the 20th of September 2022.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"141"},"PeriodicalIF":5.5000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12463772/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01561-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sepsis-induced myocardial dysfunction (SIMD) remains poorly defined due to scarce longitudinal studies with advanced echocardiography. We characterized SIMD progression using speckle tracking echocardiography (STE).
Methods: Prospective single-center study in septic shock patients admitted to intensive care. SIMD was defined as any left ventricular (LV, systolic and/or diastolic) and/or right ventricular (RV) systolic dysfunction, using STE or non-STE criteria, on days 1, 7 and 30. We studied prevalence, evolution and prognosis of SIMD classified with either criteria using Cox regression.
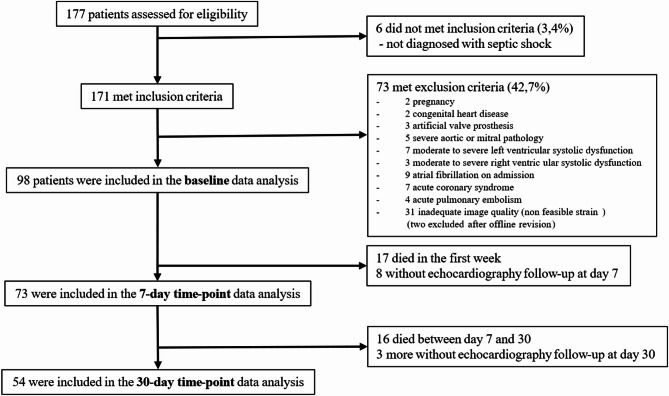
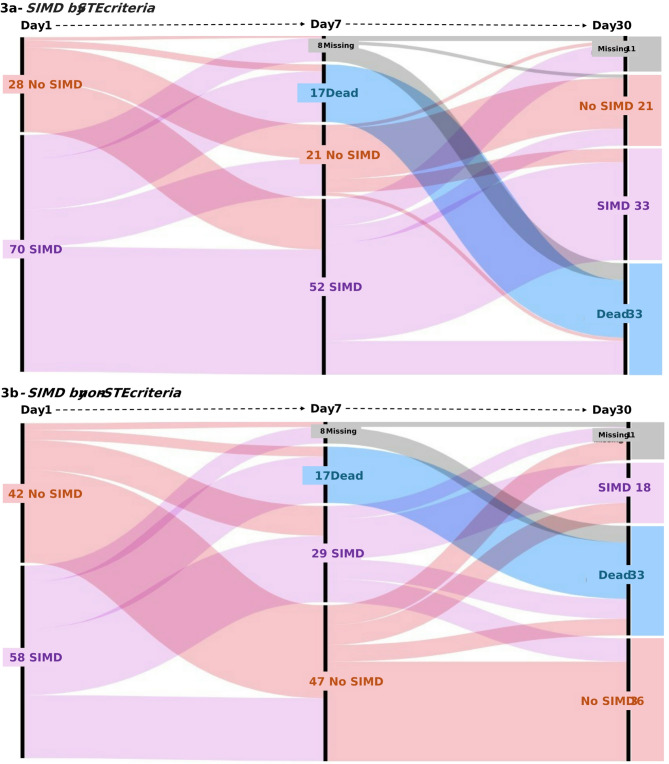
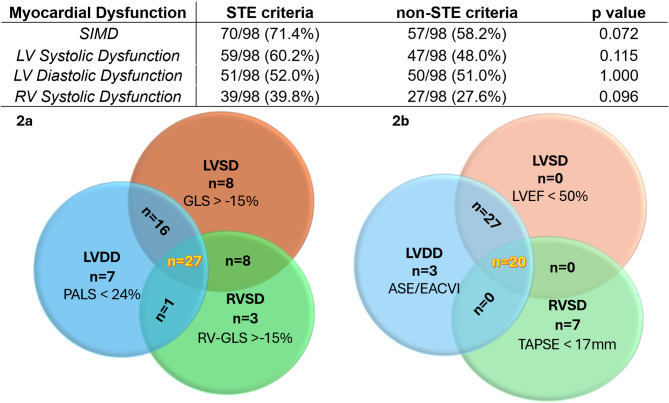
Results: Ninety-eight consecutive patients were included. On day 1, SIMD was identified in n = 57/98 (58.2%) and n = 70/98 (71.4%;p = 0.072) by non-STE and STE parameters, respectively. No significant difference in diagnosis was seen for LV diastolic dysfunction: n = 50/98 (51.0%, non-STE) vs. n = 51/98 (52.0%, STE; p = 1.00). Prevalences of LV and RV systolic dysfunction were not significantly higher with STE criteria: n = 59/98 (60.2%, STE) vs. n = 47/98 (48.0%, non-STE; p = 0.115) for LV; n = 39/98 (39.8%, STE) vs. n = 27/98 (27.6%, non-STE; p = 0.096) for RV. More patients recovered from SIMD when evaluated with non-STE criteria at day 7 (35.3% vs. 17.5% STE; p = 0.033), but not at day 30 (24.5% vs. 18.8% STE; p = 0.501). The 30-day mortality (n = 33/98, 33.7%) was associated with SIMD diagnosed using non-STE (p = 0.010), but not with STE (p = 0.057). In Cox regression, only LVDD by non-STE criteria predicted 30-day mortality (p = 0.005).
Conclusions: The incidence of SIMD in septic shock is higher when using STE criteria, with lower reversibility in the first week. A broad definition of SIMD utilizing STE criteria does not seem to provide additional prognostic value.
Trial registration: ClinicalTrials.gov: NCT05552521 registered on the 20th of September 2022.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


