Ravi B Parikh, Kristin A Linn, Junning Liang, Sae-Hwan Park, Torrey Shirk, Deborah S Cousins, Caleb Hearn, Matthew Maciejewski, Amol S Navathe
{"title":"Unfairness toward rural beneficiaries in Medicare's hierarchical conditions categories score.","authors":"Ravi B Parikh, Kristin A Linn, Junning Liang, Sae-Hwan Park, Torrey Shirk, Deborah S Cousins, Caleb Hearn, Matthew Maciejewski, Amol S Navathe","doi":"10.1093/haschl/qxaf167","DOIUrl":null,"url":null,"abstract":"<p><p>Risk adjustment is used in healthcare payment to mitigate the payer incentive to select for healthier populations and to improve fairness of quality assessment. The Centers for Medicare and Medicaid Services (CMS) has used a spending-based metric, the CMS Hierarchical Condition Category (HCC) score, to determine risk. However, the HCC score is potentially confounded by access and utilization differences, which are related to income and rurality. In this study, we investigate how related HCC scores are to mortality, a more objective indicator of clinical risk state, and whether that relationship differs between rural and urban populations. We examined calibration of the HCC spending model by calculating the predicted-to-observed spending ratio within deciles of the HCC score. We then compared urban and rural beneficiaries' clinical risk by comparing observed mortality rates within deciles. Our results demonstrate that the HCC model underpredicts mortality, while overpredicting spending, for rural beneficiaries. In contrast, it is well-calibrated for urban beneficiaries. These findings suggest that risk models based on HCCs may systematically disadvantage rural beneficiaries because HCC-based risk-adjusted spending may not fully account for baseline clinical risk.</p>","PeriodicalId":94025,"journal":{"name":"Health affairs scholar","volume":"3 9","pages":"qxaf167"},"PeriodicalIF":2.7000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12456169/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health affairs scholar","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/haschl/qxaf167","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
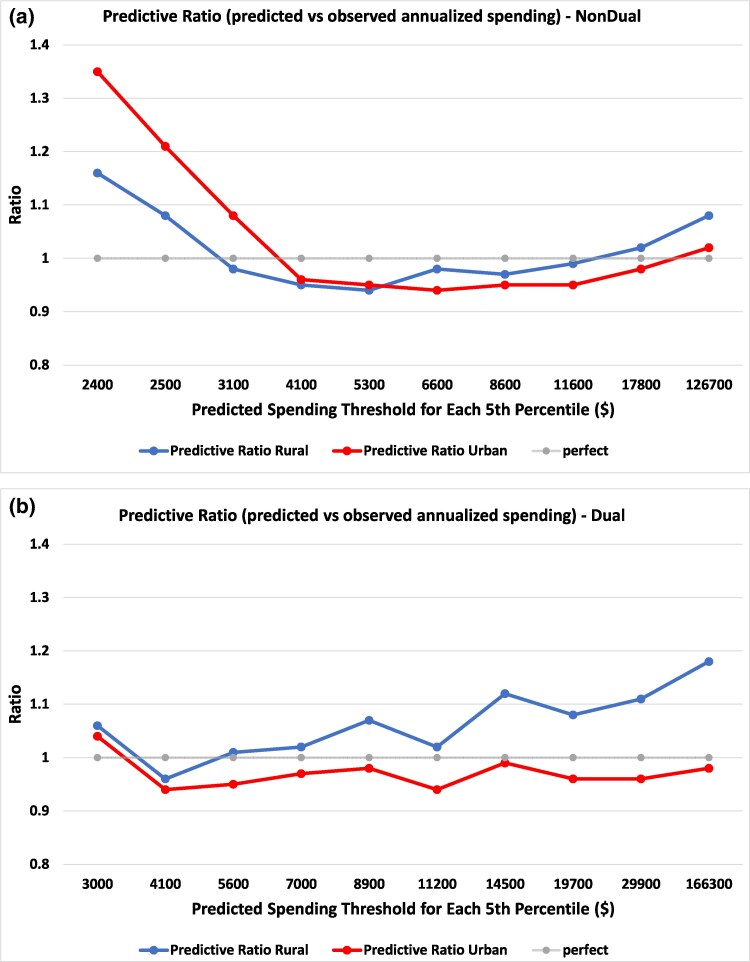
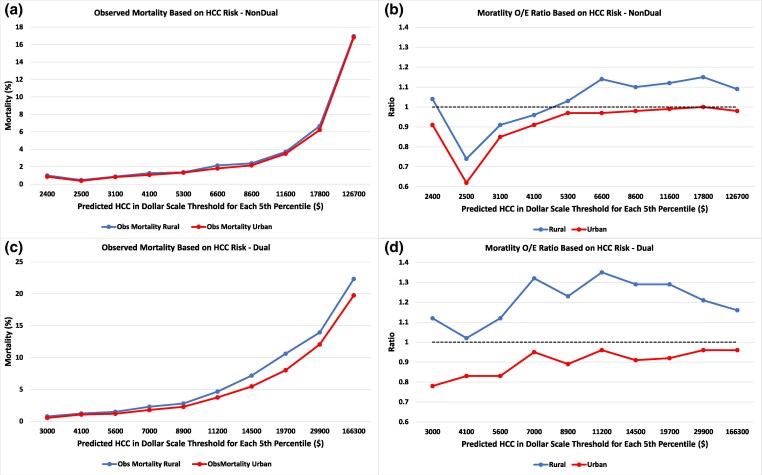
Risk adjustment is used in healthcare payment to mitigate the payer incentive to select for healthier populations and to improve fairness of quality assessment. The Centers for Medicare and Medicaid Services (CMS) has used a spending-based metric, the CMS Hierarchical Condition Category (HCC) score, to determine risk. However, the HCC score is potentially confounded by access and utilization differences, which are related to income and rurality. In this study, we investigate how related HCC scores are to mortality, a more objective indicator of clinical risk state, and whether that relationship differs between rural and urban populations. We examined calibration of the HCC spending model by calculating the predicted-to-observed spending ratio within deciles of the HCC score. We then compared urban and rural beneficiaries' clinical risk by comparing observed mortality rates within deciles. Our results demonstrate that the HCC model underpredicts mortality, while overpredicting spending, for rural beneficiaries. In contrast, it is well-calibrated for urban beneficiaries. These findings suggest that risk models based on HCCs may systematically disadvantage rural beneficiaries because HCC-based risk-adjusted spending may not fully account for baseline clinical risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


