Timing matters: overall treatment time, radiotherapy interruptions, and outcomes in glioblastomas-prognostic significance in different biological sub-groups.
Paolo Tini, Flavio Donnini, Francesco Marampon, Pierpaolo Pastina, Giovanni Rubino, Giuseppe Battaglia, Salvatore Chibbaro, Alfonso Cerase, Maria Antonietta Mazzei, Isacco Desideri, Giuseppe Minniti
{"title":"Timing matters: overall treatment time, radiotherapy interruptions, and outcomes in glioblastomas-prognostic significance in different biological sub-groups.","authors":"Paolo Tini, Flavio Donnini, Francesco Marampon, Pierpaolo Pastina, Giovanni Rubino, Giuseppe Battaglia, Salvatore Chibbaro, Alfonso Cerase, Maria Antonietta Mazzei, Isacco Desideri, Giuseppe Minniti","doi":"10.1007/s11060-025-05215-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Glioblastoma (GBM) is the most common and aggressive primary malignant brain tumor in adults, with a median overall survival (OS) rarely exceeding 15 months despite multimodal therapy. While established prognostic factors include age, Karnofsky Performance Status (KPS), and molecular features such as MGMT promoter methylation and IDH mutation status, increasing attention has focused on the role of treatment timing as a potentially modifiable prognostic determinant. In particular, Overall Treatment Time (OTT)-the number of calendar days from the first to the last radiotherapy fraction-may impact survival by enabling tumor repopulation when extended or interrupted.</p><p><strong>Methods: </strong>We conducted a retrospective monocentric cohort study of 166 consecutive adult patients with histologically confirmed IDH-wild-type glioblastoma treated with standard concurrent chemoradiotherapy and adjuvant temozolomide between January 2016 and January 2024. OTT was defined as the total number of days from radiotherapy start to end, including all interruptions. A cutoff of 48 days was adopted based on prior evidence. Patients were stratified according to OTT, number and cause of radiotherapy interruptions, and molecular status (MGMT promoter methylation and EGFR amplification). The primary endpoints were OS and progression-free survival (PFS), analyzed with Kaplan-Meier and Cox regression models.</p><p><strong>Results: </strong>Median OTT was 43 days (range: 40-65). Patients with OTT ≤ 48 days had a significantly longer median OS than those with OTT > 48 days (20 vs. 10 months, p = 0.003). Multivariable Cox regression confirmed OTT > 48 days as an independent negative prognostic factor (HR = 1.41, p = 0.009). Multiple interruptions, regardless of cause, further reduced OS, particularly in patients with MGMT-methylated tumors and low EGFR expression. Clinical interruptions-often due to toxicity-were associated with significantly worse outcomes than single technical interruptions. Notably, the negative impact of prolonged OTT was significantly more pronounced in the MGMT-methylated subgroup (p for interaction = 0.018), suggesting a biologically distinct vulnerability to treatment delays.</p><p><strong>Conclusions: </strong>This study demonstrates that prolonged OTT and radiotherapy interruptions are independently associated with inferior survival in patients with IDH-wild-type glioblastoma, particularly in biologically favorable subgroups such as MGMT-methylated tumors. These findings underscore the importance of strict adherence to treatment schedules and minimizing avoidable delays. Molecular profiling may aid in identifying patients most vulnerable to the adverse effects of treatment prolongation, supporting a more personalized and time-sensitive approach to GBM management. Further prospective validation is warranted.</p>","PeriodicalId":16425,"journal":{"name":"Journal of Neuro-Oncology","volume":" ","pages":"1261-1269"},"PeriodicalIF":3.1000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12511268/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neuro-Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11060-025-05215-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Glioblastoma (GBM) is the most common and aggressive primary malignant brain tumor in adults, with a median overall survival (OS) rarely exceeding 15 months despite multimodal therapy. While established prognostic factors include age, Karnofsky Performance Status (KPS), and molecular features such as MGMT promoter methylation and IDH mutation status, increasing attention has focused on the role of treatment timing as a potentially modifiable prognostic determinant. In particular, Overall Treatment Time (OTT)-the number of calendar days from the first to the last radiotherapy fraction-may impact survival by enabling tumor repopulation when extended or interrupted.
Methods: We conducted a retrospective monocentric cohort study of 166 consecutive adult patients with histologically confirmed IDH-wild-type glioblastoma treated with standard concurrent chemoradiotherapy and adjuvant temozolomide between January 2016 and January 2024. OTT was defined as the total number of days from radiotherapy start to end, including all interruptions. A cutoff of 48 days was adopted based on prior evidence. Patients were stratified according to OTT, number and cause of radiotherapy interruptions, and molecular status (MGMT promoter methylation and EGFR amplification). The primary endpoints were OS and progression-free survival (PFS), analyzed with Kaplan-Meier and Cox regression models.
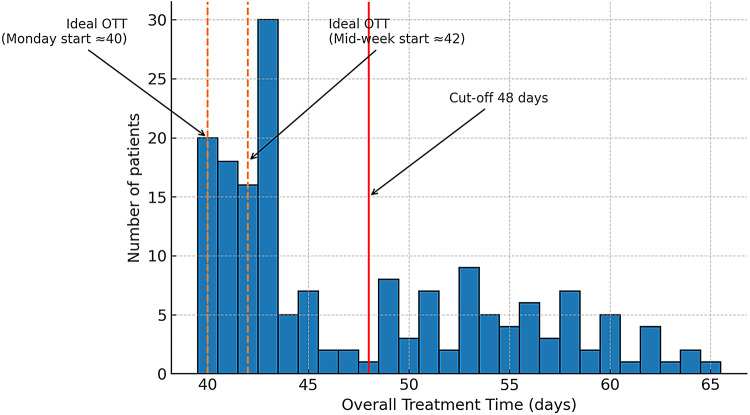
Results: Median OTT was 43 days (range: 40-65). Patients with OTT ≤ 48 days had a significantly longer median OS than those with OTT > 48 days (20 vs. 10 months, p = 0.003). Multivariable Cox regression confirmed OTT > 48 days as an independent negative prognostic factor (HR = 1.41, p = 0.009). Multiple interruptions, regardless of cause, further reduced OS, particularly in patients with MGMT-methylated tumors and low EGFR expression. Clinical interruptions-often due to toxicity-were associated with significantly worse outcomes than single technical interruptions. Notably, the negative impact of prolonged OTT was significantly more pronounced in the MGMT-methylated subgroup (p for interaction = 0.018), suggesting a biologically distinct vulnerability to treatment delays.
Conclusions: This study demonstrates that prolonged OTT and radiotherapy interruptions are independently associated with inferior survival in patients with IDH-wild-type glioblastoma, particularly in biologically favorable subgroups such as MGMT-methylated tumors. These findings underscore the importance of strict adherence to treatment schedules and minimizing avoidable delays. Molecular profiling may aid in identifying patients most vulnerable to the adverse effects of treatment prolongation, supporting a more personalized and time-sensitive approach to GBM management. Further prospective validation is warranted.
期刊介绍:
The Journal of Neuro-Oncology is a multi-disciplinary journal encompassing basic, applied, and clinical investigations in all research areas as they relate to cancer and the central nervous system. It provides a single forum for communication among neurologists, neurosurgeons, radiotherapists, medical oncologists, neuropathologists, neurodiagnosticians, and laboratory-based oncologists conducting relevant research. The Journal of Neuro-Oncology does not seek to isolate the field, but rather to focus the efforts of many disciplines in one publication through a format which pulls together these diverse interests. More than any other field of oncology, cancer of the central nervous system requires multi-disciplinary approaches. To alleviate having to scan dozens of journals of cell biology, pathology, laboratory and clinical endeavours, JNO is a periodical in which current, high-quality, relevant research in all aspects of neuro-oncology may be found.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


