A Comparison of Single Dose Remimazolam With Dexmedetomidine for the Prevention of Emergence Delirium in Children Undergoing Tonsillectomy and Adenoidectomy Surgery Under Sevoflurane Anesthesia: A Randomized Clinical Trial.
{"title":"A Comparison of Single Dose Remimazolam With Dexmedetomidine for the Prevention of Emergence Delirium in Children Undergoing Tonsillectomy and Adenoidectomy Surgery Under Sevoflurane Anesthesia: A Randomized Clinical Trial.","authors":"Ting Liu, Jing Zhou, Xi-Xi Wang, Si-Fei Gan, Jie-Qiong Liu, Peng-Fei Zhu, Mei-Hong Li, Fang Luo","doi":"10.1155/anrp/7780635","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Emergence delirium, characterized by early postoperative behavioral changes in pediatric patients, poses potential risks to patient safety, resulting in extended hospital stays and increased medical costs. Remimazolam has a rapid onset, moderate half-life, and lower compression on respiratory and circulatory function. This double-blind randomized study aims to compare the incidence of emergence delirium in pediatric patients who received a single dose of remimazolam or dexmedetomidine before the end of sevoflurane anesthesia. <b>Methods:</b> A total of 110 pediatric patients aged 2-12 years, American Society of Anesthesiologists (ASA) Class I or II, undergoing elective tonsillectomy and adenoidectomy were included in this study and randomized into the dexmedetomidine group and remimazolam group (R group) (<i>n</i> = 55). Inhalation of sevoflurane was stopped 15 min before surgery after asking the surgeon's opinion, and either 0.2 mg/kg of remimazolam or 0.2 μg/kg of dexmedetomidine was administered. The main and secondary results of the research were both analyzed with the intention-to-treat analysis. The main outcome observed in this study was the incidence of emergence delirium in both groups. Secondary outcomes were vital signs at various time points after administration, Pediatric Anesthesia Emergence Delirium (PAED) scale score for delirium, extubation time, the length of time in the postanesthesia care unit (PACU), postoperative adverse events, and parental satisfaction. <b>Results:</b> The intention-to-treat analysis indicated that the mean age of patients was 5.7 ± 0.4 years, with 62 (56.4%) of them being male. The incidence of emergence delirium was 25.5% overall, with no significant difference seen between the two groups. Compared to the R group, dexmedetomidine decreased the heart rate significantly (<i>p</i> < 0.001). There were no differences in extubation time, PACU stay, postoperative adverse events, and parental satisfaction between the two groups. In addition, age is an independent risk factor contributing to the emergence delirium. <b>Conclusions:</b> Discontinuing the inhalation of sevoflurane 15 min before the end of the procedure and administering 0.2 mg/kg of remimazolam intravenously did not show superiority over 0.2 μg/kg of dexmedetomidine in preventing emergence delirium. <b>Trial Registration:</b> Chinese Registry of Clinical Trials: ChiCTR2300072526.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2025 ","pages":"7780635"},"PeriodicalIF":1.3000,"publicationDate":"2025-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450552/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/anrp/7780635","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
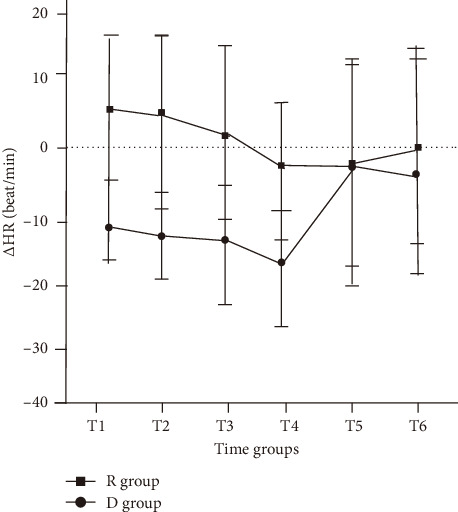
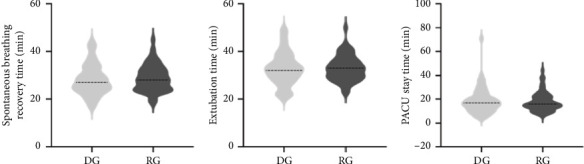
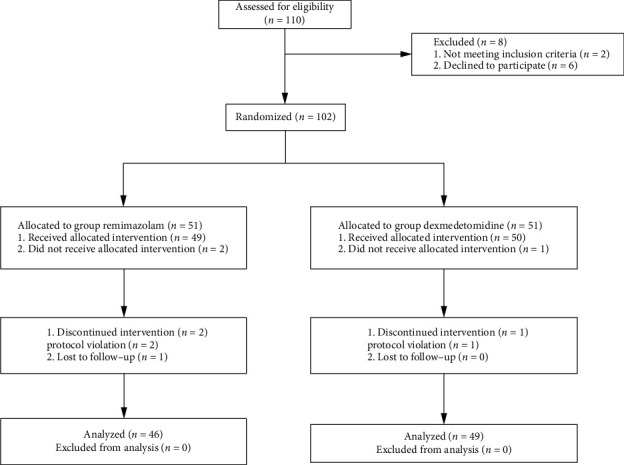
Introduction: Emergence delirium, characterized by early postoperative behavioral changes in pediatric patients, poses potential risks to patient safety, resulting in extended hospital stays and increased medical costs. Remimazolam has a rapid onset, moderate half-life, and lower compression on respiratory and circulatory function. This double-blind randomized study aims to compare the incidence of emergence delirium in pediatric patients who received a single dose of remimazolam or dexmedetomidine before the end of sevoflurane anesthesia. Methods: A total of 110 pediatric patients aged 2-12 years, American Society of Anesthesiologists (ASA) Class I or II, undergoing elective tonsillectomy and adenoidectomy were included in this study and randomized into the dexmedetomidine group and remimazolam group (R group) (n = 55). Inhalation of sevoflurane was stopped 15 min before surgery after asking the surgeon's opinion, and either 0.2 mg/kg of remimazolam or 0.2 μg/kg of dexmedetomidine was administered. The main and secondary results of the research were both analyzed with the intention-to-treat analysis. The main outcome observed in this study was the incidence of emergence delirium in both groups. Secondary outcomes were vital signs at various time points after administration, Pediatric Anesthesia Emergence Delirium (PAED) scale score for delirium, extubation time, the length of time in the postanesthesia care unit (PACU), postoperative adverse events, and parental satisfaction. Results: The intention-to-treat analysis indicated that the mean age of patients was 5.7 ± 0.4 years, with 62 (56.4%) of them being male. The incidence of emergence delirium was 25.5% overall, with no significant difference seen between the two groups. Compared to the R group, dexmedetomidine decreased the heart rate significantly (p < 0.001). There were no differences in extubation time, PACU stay, postoperative adverse events, and parental satisfaction between the two groups. In addition, age is an independent risk factor contributing to the emergence delirium. Conclusions: Discontinuing the inhalation of sevoflurane 15 min before the end of the procedure and administering 0.2 mg/kg of remimazolam intravenously did not show superiority over 0.2 μg/kg of dexmedetomidine in preventing emergence delirium. Trial Registration: Chinese Registry of Clinical Trials: ChiCTR2300072526.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


