The temporal trends of ST-elevation myocardial infarction mortality according to infarct size and location: insights from the UK National MINAP registry from 2005 to 2019.
Nicholas Weight, Rodrigo Bagur, Nicholas Chew, Sripal Bangalore, Purvi Parwani, Louise Y Sun, Yu Chen Wang, Muhammad Rashid, Mamas A Mamas
{"title":"The temporal trends of ST-elevation myocardial infarction mortality according to infarct size and location: insights from the UK National MINAP registry from 2005 to 2019.","authors":"Nicholas Weight, Rodrigo Bagur, Nicholas Chew, Sripal Bangalore, Purvi Parwani, Louise Y Sun, Yu Chen Wang, Muhammad Rashid, Mamas A Mamas","doi":"10.1093/ehjopen/oeaf111","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Myocardial infarction size is associated with mortality in ST-elevation myocardial infarction (STEMI). With advances in primary percutaneous coronary intervention (PPCI) and medical therapy, whether this relationship has changed over time is unclear.</p><p><strong>Methods and results: </strong>Patients with STEMI in the UK from 2005 to 2019 were included from the national AMI MINAP registry, with mortality linkage to 2021. Primary outcomes were all-cause mortality at 30 days and 1 year according to infarct size, using Cox regression models. Infarct size was stratified by Tertiles (T1-3) of peak troponin level (T1, smallest; T3, largest), across the early (2005-09), middle (2010-14), and late (2015-19) periods. Subgroup analyses assessed the relationship according to infarct location (anterior vs. non-anterior). A total of 177 214 STEMI patients were included. Adjusted 30-day mortality risk according to infarct size was highest in the early period (aHR: 1.32, 1.21-1.45, <i>P</i> < 0.001), compared to middle (1.12, 1.04-1.20, <i>P</i> = 0.002) and late study periods (1.05, 0.96-1.14, <i>P</i> = 0.299). The relationship between infarct size and 30-day mortality was significant for patients with anterior STEMI in early (1.39, 1.22-1.57, <i>P</i> < 0.001) but not middle or late periods, while remained significant for non-anterior infarction until the late period (early, 1.28, 1.13-1.45, <i>P</i> < 0.001; middle, 1.17, 1.06-1.29, <i>P</i> = 0.002; late, 1.09, 0.96-1.24, <i>P</i> = 0.180).</p><p><strong>Conclusion: </strong>We observed an independent relationship between infarct size and STEMI mortality, strongest between 2005 and 2009, which reduced over time, becoming non-significant in the 2015-19 period. This association diminished more rapidly for patients with anterior STEMIs. These findings underscore the potential role of contemporary revascularization, systems of care, and guideline-directed medical therapy in reducing STEMI-related mortality.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 5","pages":"oeaf111"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12448480/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf111","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Myocardial infarction size is associated with mortality in ST-elevation myocardial infarction (STEMI). With advances in primary percutaneous coronary intervention (PPCI) and medical therapy, whether this relationship has changed over time is unclear.
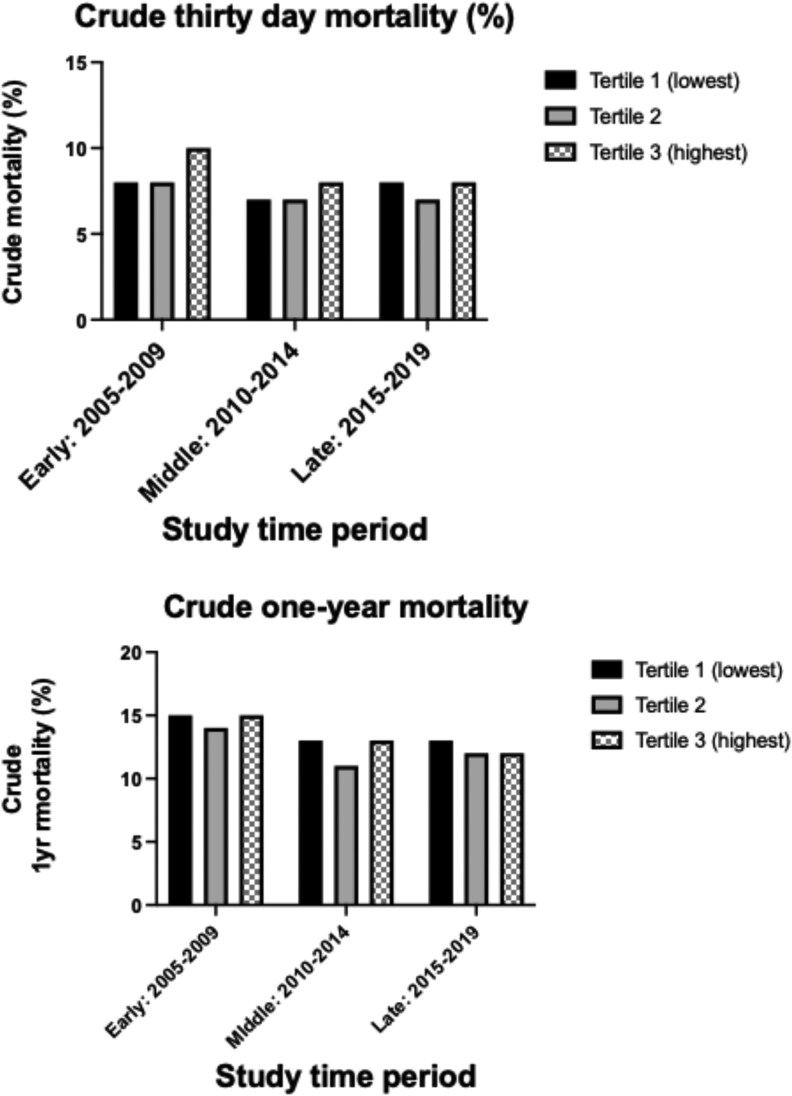
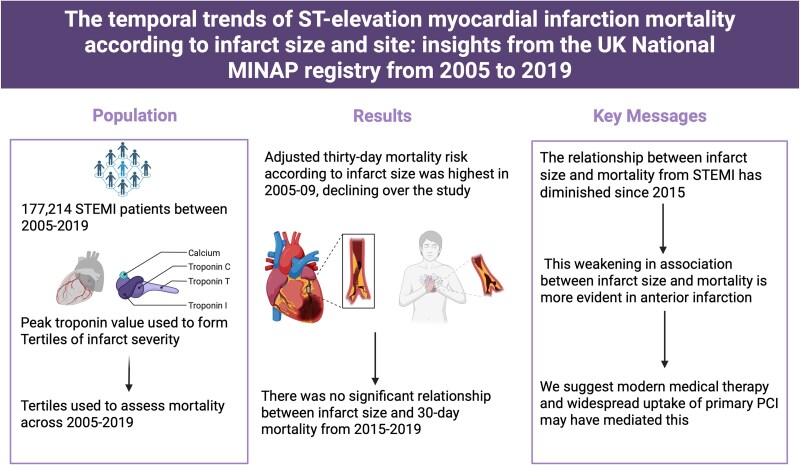
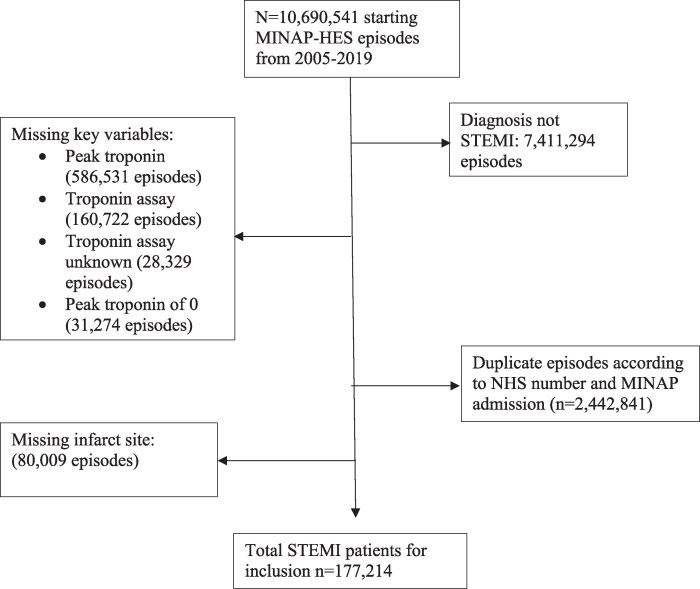
Methods and results: Patients with STEMI in the UK from 2005 to 2019 were included from the national AMI MINAP registry, with mortality linkage to 2021. Primary outcomes were all-cause mortality at 30 days and 1 year according to infarct size, using Cox regression models. Infarct size was stratified by Tertiles (T1-3) of peak troponin level (T1, smallest; T3, largest), across the early (2005-09), middle (2010-14), and late (2015-19) periods. Subgroup analyses assessed the relationship according to infarct location (anterior vs. non-anterior). A total of 177 214 STEMI patients were included. Adjusted 30-day mortality risk according to infarct size was highest in the early period (aHR: 1.32, 1.21-1.45, P < 0.001), compared to middle (1.12, 1.04-1.20, P = 0.002) and late study periods (1.05, 0.96-1.14, P = 0.299). The relationship between infarct size and 30-day mortality was significant for patients with anterior STEMI in early (1.39, 1.22-1.57, P < 0.001) but not middle or late periods, while remained significant for non-anterior infarction until the late period (early, 1.28, 1.13-1.45, P < 0.001; middle, 1.17, 1.06-1.29, P = 0.002; late, 1.09, 0.96-1.24, P = 0.180).
Conclusion: We observed an independent relationship between infarct size and STEMI mortality, strongest between 2005 and 2009, which reduced over time, becoming non-significant in the 2015-19 period. This association diminished more rapidly for patients with anterior STEMIs. These findings underscore the potential role of contemporary revascularization, systems of care, and guideline-directed medical therapy in reducing STEMI-related mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


