Improvement in global longitudinal strain following plasma cell-directed therapy is associated with long-term survival among patients with AL amyloidosis.
Kristine H Jang, Anthony F Yu, Heather Landau, Xiaoyue Ma, Richard K Cheng, Mathew S Mauer, Katherine Lee Chuy, Daniel Lenihan, Ji Can Yang, Carol L Chen, Jennifer E Liu
{"title":"Improvement in global longitudinal strain following plasma cell-directed therapy is associated with long-term survival among patients with AL amyloidosis.","authors":"Kristine H Jang, Anthony F Yu, Heather Landau, Xiaoyue Ma, Richard K Cheng, Mathew S Mauer, Katherine Lee Chuy, Daniel Lenihan, Ji Can Yang, Carol L Chen, Jennifer E Liu","doi":"10.1093/ehjopen/oeaf104","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cardiac impairment in AL amyloidosis is the major determinant of survival. Treatment goals include reducing circulating light chains to improve organ function. Global longitudinal strain (GLS) is an independent predictor of survival and useful for assessing cardiac function before and after therapy. This study aimed to describe GLS change from baseline to one year post-treatment, identify factors associated with GLS improvement (GLS+), and evaluate its prognostic significance.</p><p><strong>Methods and results: </strong>Ninety-seven patients with AL amyloidosis and cardiac stage II/III disease who underwent echocardiogram and haematologic evaluation at baseline and one year were included. GLS+ was defined as a 2.0%-point increase. A cardiac or B-type natriuretic peptide (BNP+) response was defined as a 30% reduction from baseline. Overall survival was measured from baseline echocardiogram to death. Of 97 patients, 62% had Stage II, 29% Stage IIIa, and 9% Stage IIIb disease. Baseline median left ventricular ejection fraction, GLS, and septal thickness were 65%, -14.9%, and 1.3 cm, respectively. GLS+ was observed in 36% of patients and BNP+ in 51%. Median overall survival was 113.4 months. The hazard ratio for survival was 0.42 in the GLS+ group and 0.46 in the BNP+ group, after adjusting for haematologic response.</p><p><strong>Conclusion: </strong>GLS improvement post-treatment confers a significant survival benefit. This study supports GLS as an important marker for risk stratification and cardiac response.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 5","pages":"oeaf104"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449083/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf104","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
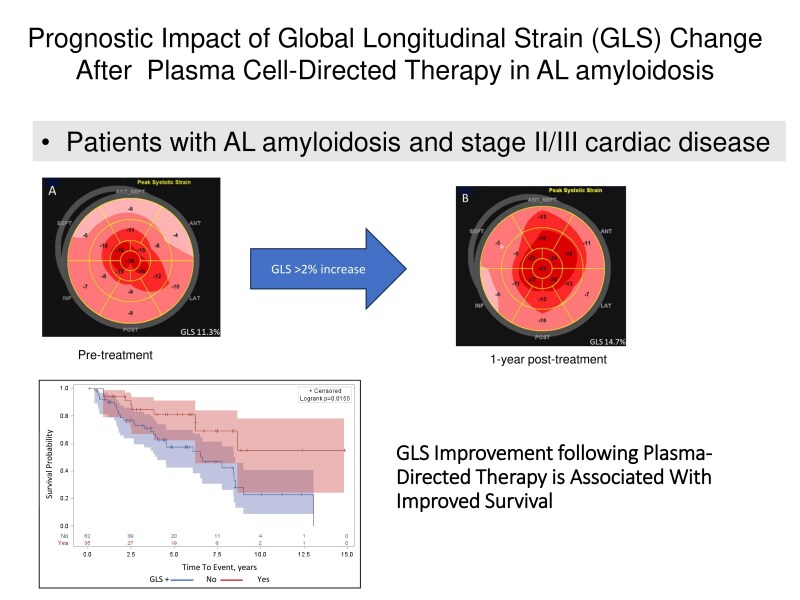
Aims: Cardiac impairment in AL amyloidosis is the major determinant of survival. Treatment goals include reducing circulating light chains to improve organ function. Global longitudinal strain (GLS) is an independent predictor of survival and useful for assessing cardiac function before and after therapy. This study aimed to describe GLS change from baseline to one year post-treatment, identify factors associated with GLS improvement (GLS+), and evaluate its prognostic significance.
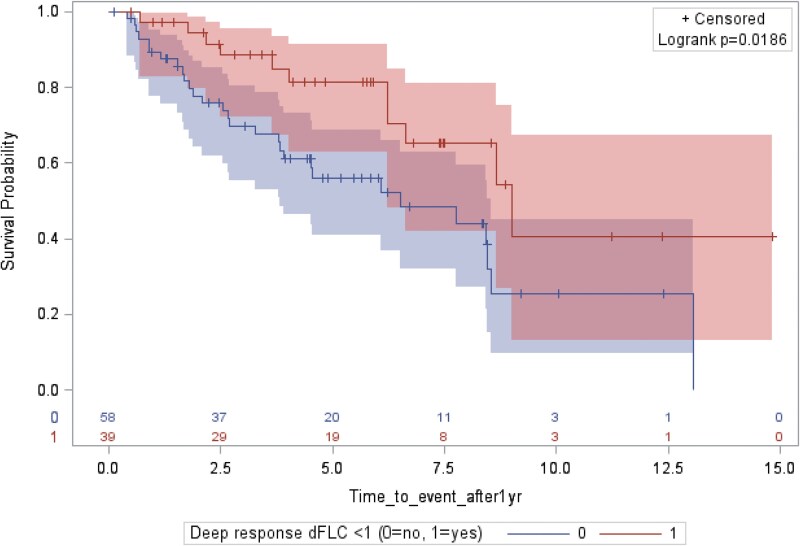
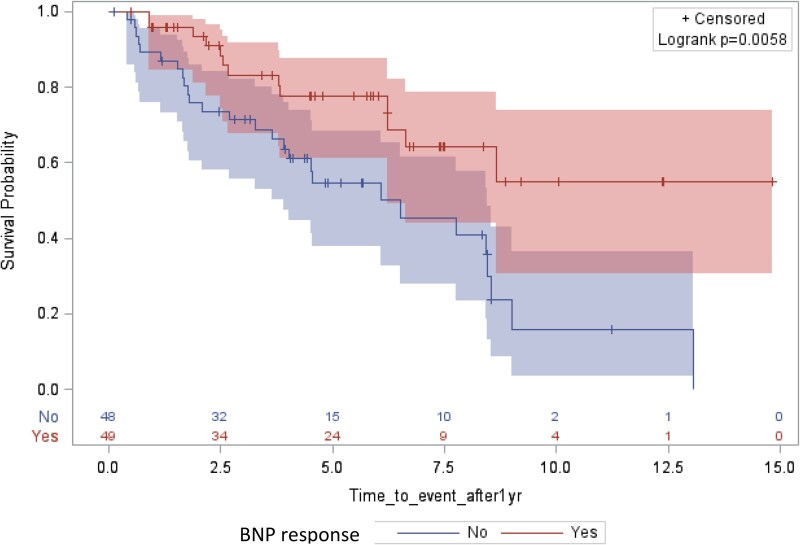
Methods and results: Ninety-seven patients with AL amyloidosis and cardiac stage II/III disease who underwent echocardiogram and haematologic evaluation at baseline and one year were included. GLS+ was defined as a 2.0%-point increase. A cardiac or B-type natriuretic peptide (BNP+) response was defined as a 30% reduction from baseline. Overall survival was measured from baseline echocardiogram to death. Of 97 patients, 62% had Stage II, 29% Stage IIIa, and 9% Stage IIIb disease. Baseline median left ventricular ejection fraction, GLS, and septal thickness were 65%, -14.9%, and 1.3 cm, respectively. GLS+ was observed in 36% of patients and BNP+ in 51%. Median overall survival was 113.4 months. The hazard ratio for survival was 0.42 in the GLS+ group and 0.46 in the BNP+ group, after adjusting for haematologic response.
Conclusion: GLS improvement post-treatment confers a significant survival benefit. This study supports GLS as an important marker for risk stratification and cardiac response.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


