Umbilical Cord Blood Sampling for Newborn Screening of Pompe Disease and the Detection of a Novel Pathogenic Variant and Pseudodeficiency Variants in an Asian Population.
Fook-Choe Cheah, Sharifah Azween Syed Omar, Jasmine Lee, Zheng Jiet Ang, Anu Ratha Gopal, Wan Nurulhuda Wan Md Zin, Beng Kwang Ng, Shu-Chuan Chiang, Yin-Hsiu Chien
{"title":"Umbilical Cord Blood Sampling for Newborn Screening of Pompe Disease and the Detection of a Novel Pathogenic Variant and Pseudodeficiency Variants in an Asian Population.","authors":"Fook-Choe Cheah, Sharifah Azween Syed Omar, Jasmine Lee, Zheng Jiet Ang, Anu Ratha Gopal, Wan Nurulhuda Wan Md Zin, Beng Kwang Ng, Shu-Chuan Chiang, Yin-Hsiu Chien","doi":"10.3390/ijns11030074","DOIUrl":null,"url":null,"abstract":"<p><p>Pompe disease is an autosomal recessive metabolic disorder caused by acid alpha-glucosidase (GAA) deficiency. The use of umbilical cord blood (UCB) for newborn screening (NBS) of Pompe disease, compared to heel-prick sampling, has not been widely studied. This study compared GAA activity in UCB from term newborns with peripheral or heel-prick blood samples obtained on days 1, 2, and 3 after birth. Enzyme assays were performed using UPLC-MS/MS. Sanger sequencing was conducted in infants with low GAA activity to identify pathogenic variants. Among 4091 UCB samples analyzed over 18 months, the mean GAA activity was 10.04 ± 5.95 μM/h, higher in females than males [Median (IQR): 9.83 (5.45) vs. 9.08 (4.97) μM/h, respectively, <i>p</i> < 0.001], and similar across ethnicities. GAA levels in UCB and Day 3 heel-prick samples were comparable. A GAA cut-off value of 1.54 μM/h (0.1% of study population) identified one infant (0.024% prevalence) with a novel bi-allelic variant-c.2005_2010del (p.Pro669_Phe670del) and c.1123C>T (p.Arg375Cys), and 12 infants with non-pathogenic pseudodeficiency alleles. This study supports GAA measurement in UCB as a viable alternative for NBS, with enzyme activity remaining stable for up to 72 h post-collection. Larger-scale multicenter nationwide studies are warranted to confirm this prevalence in our population.</p>","PeriodicalId":14159,"journal":{"name":"International Journal of Neonatal Screening","volume":"11 3","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12452700/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Neonatal Screening","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/ijns11030074","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
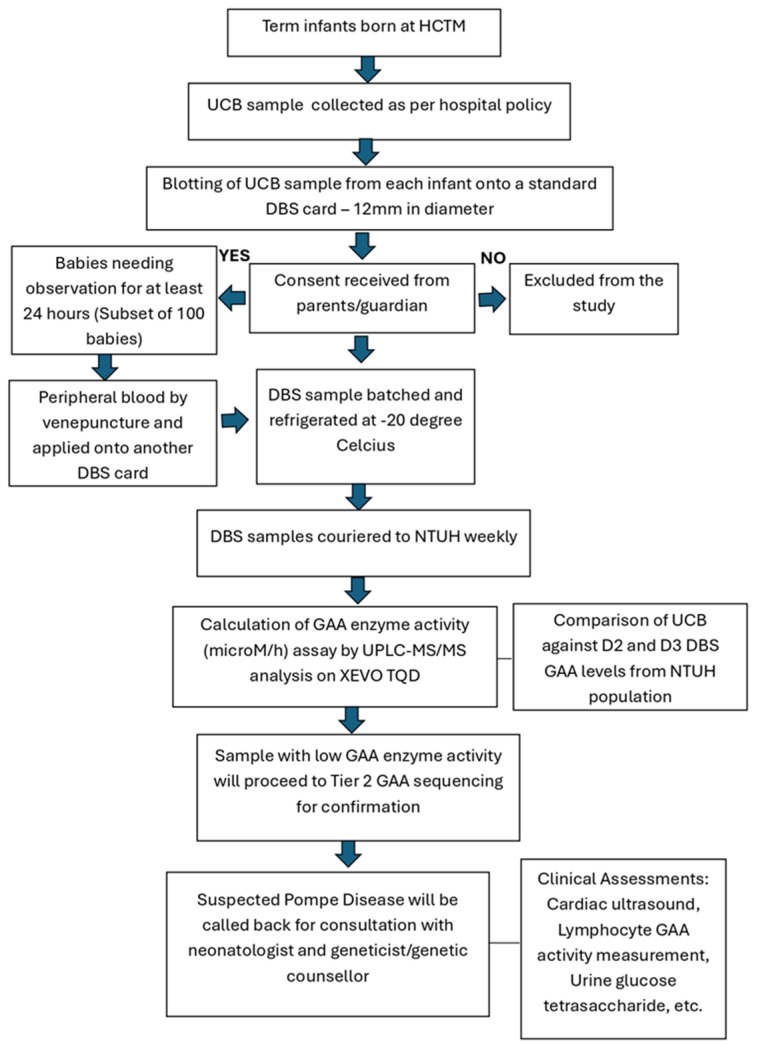
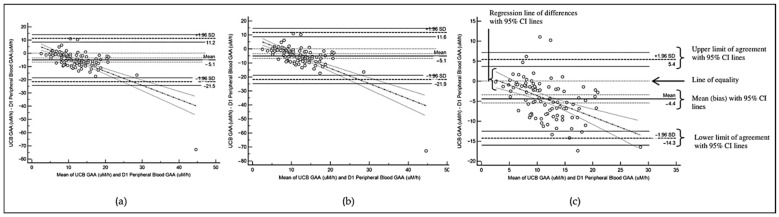
Pompe disease is an autosomal recessive metabolic disorder caused by acid alpha-glucosidase (GAA) deficiency. The use of umbilical cord blood (UCB) for newborn screening (NBS) of Pompe disease, compared to heel-prick sampling, has not been widely studied. This study compared GAA activity in UCB from term newborns with peripheral or heel-prick blood samples obtained on days 1, 2, and 3 after birth. Enzyme assays were performed using UPLC-MS/MS. Sanger sequencing was conducted in infants with low GAA activity to identify pathogenic variants. Among 4091 UCB samples analyzed over 18 months, the mean GAA activity was 10.04 ± 5.95 μM/h, higher in females than males [Median (IQR): 9.83 (5.45) vs. 9.08 (4.97) μM/h, respectively, p < 0.001], and similar across ethnicities. GAA levels in UCB and Day 3 heel-prick samples were comparable. A GAA cut-off value of 1.54 μM/h (0.1% of study population) identified one infant (0.024% prevalence) with a novel bi-allelic variant-c.2005_2010del (p.Pro669_Phe670del) and c.1123C>T (p.Arg375Cys), and 12 infants with non-pathogenic pseudodeficiency alleles. This study supports GAA measurement in UCB as a viable alternative for NBS, with enzyme activity remaining stable for up to 72 h post-collection. Larger-scale multicenter nationwide studies are warranted to confirm this prevalence in our population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


