{"title":"Effect of prehabilitation on postoperative outcomes in patients with upper gastrointestinal tract cancer: meta-analysis.","authors":"Qi Li, Jianhong Liu, Liqing Li, Yeli Luo","doi":"10.1093/bjsopen/zraf091","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of this meta-analysis was to elucidate the effects of prehabilitation (PR) on outcomes after surgery for upper gastrointestinal tract cancer.</p><p><strong>Methods: </strong>PubMed, Web of Science, Embase, and Cochrane databases were searched from inception up to 21 May 2024 for randomized clinical trials (RCTs) and cohort studies investigating PR interventions in patients with upper gastrointestinal tract cancer. Data were synthesized using standardized mean differences (SMDs) and risk ratios (RRs) with corresponding 95% confidence intervals. Sensitivity and subgroup analyses were used to examine the robustness of the results and find possible sources of heterogeneity. Statistical analyses were performed using Review Manager 5.4 and Stata 16.0.</p><p><strong>Results: </strong>Eight RCTs and eight cohort studies were included in the meta-analysis. Compared with the control group (no PR), the PR group had a significantly shorter postoperative length of hospital stay (SMD -0.27; 95% confidence interval (c.i.) -0.47 to -0.07; P = 0.008), a significant reduction in the occurrence of pneumonia after the surgery (RR 0.71; 95% c.i. 0.50 to 1.00; P = 0.005), and a greater improvement in the 6-minute walk distance (SMD 0.95; 95% c.i. 0.68 to 1.22; P < 0.00001). However, there were no significant differences between the control and PR groups in overall postoperative complications, anastomotic leakage, overall pulmonary complications, operative time, intraoperative blood loss, wound infection rate, in-hospital mortality, or recurrence rate (all P > 0.05).</p><p><strong>Conclusion: </strong>For the population with upper gastrointestinal tract cancer, PR can partially lower the risk of postoperative pneumonia and promote faster postoperative recovery. Given the inherent limitations in the included studies, more large-scale RCTs are needed to verify these findings.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"9 5","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12452279/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zraf091","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The aim of this meta-analysis was to elucidate the effects of prehabilitation (PR) on outcomes after surgery for upper gastrointestinal tract cancer.
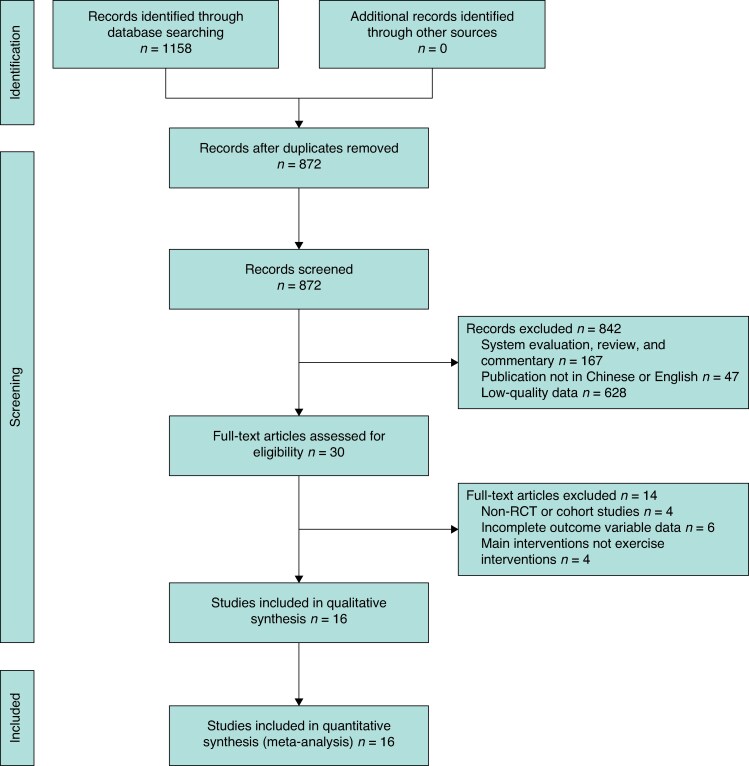
Methods: PubMed, Web of Science, Embase, and Cochrane databases were searched from inception up to 21 May 2024 for randomized clinical trials (RCTs) and cohort studies investigating PR interventions in patients with upper gastrointestinal tract cancer. Data were synthesized using standardized mean differences (SMDs) and risk ratios (RRs) with corresponding 95% confidence intervals. Sensitivity and subgroup analyses were used to examine the robustness of the results and find possible sources of heterogeneity. Statistical analyses were performed using Review Manager 5.4 and Stata 16.0.
Results: Eight RCTs and eight cohort studies were included in the meta-analysis. Compared with the control group (no PR), the PR group had a significantly shorter postoperative length of hospital stay (SMD -0.27; 95% confidence interval (c.i.) -0.47 to -0.07; P = 0.008), a significant reduction in the occurrence of pneumonia after the surgery (RR 0.71; 95% c.i. 0.50 to 1.00; P = 0.005), and a greater improvement in the 6-minute walk distance (SMD 0.95; 95% c.i. 0.68 to 1.22; P < 0.00001). However, there were no significant differences between the control and PR groups in overall postoperative complications, anastomotic leakage, overall pulmonary complications, operative time, intraoperative blood loss, wound infection rate, in-hospital mortality, or recurrence rate (all P > 0.05).
Conclusion: For the population with upper gastrointestinal tract cancer, PR can partially lower the risk of postoperative pneumonia and promote faster postoperative recovery. Given the inherent limitations in the included studies, more large-scale RCTs are needed to verify these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


