Justin R Zhu, Ismail Ajjawi, Wesley Day, Michael J Gouzoulis, Anthony Seddio, Jonathan N Grauer
{"title":"The Correlation of Surgeon Subspecialty With Outcomes Following Surgery for Geriatric Femoral Neck Fracture.","authors":"Justin R Zhu, Ismail Ajjawi, Wesley Day, Michael J Gouzoulis, Anthony Seddio, Jonathan N Grauer","doi":"10.5435/JAAOSGlobal-D-25-00103","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Geriatric femoral neck fractures are common and typically managed with hemiarthroplasty (HA), total hip arthroplasty (THA), or percutaneous pinning (PP) by an on-call physician. The current study assessed if perioperative or longer-term outcomes correlated with orthopaedic surgeon subspecialty.</p><p><strong>Methods: </strong>The 2016 to 2022 PearlDiver M161 Ortho administrative data set was used to identify patients >65 years who underwent HA, THA, or PP for femoral neck fracture. The subspecialty of the treating surgeon was defined as arthroplasty, trauma, or nonarthroplasty/nontrauma. Exclusion criteria included polytrauma and concurrent neoplasms/infections. For each surgery type, 90-day perioperative adverse events were assessed between surgeon cohorts using multivariate logistic regression. Five-year revisions/dislocations were also assessed.</p><p><strong>Results: </strong>Overall, 150,728 surgeries were identified (140,850 by nontrauma/nonarthroplasty surgeons, 5,013 arthroplasty, and 4,865 trauma). Arthroplasty surgeons performed THA at higher rates than trauma or nonarthroplasty/nontrauma surgeons (28.1% versus 7.7% and 12.8%, respectively, P < 0.001). Ninety-day outcomes were more similar than different across surgeon specialties. For HA, 5-year dislocation rates were statistically different but within 1% between cohorts (nonarthroplasty/nontrauma 97.5%, arthroplasty 96.8%, trauma 97.8%). Five-year revision rates were also within 1% between the cohorts (nonarthroplasty/nontrauma 98.2%, arthroplasty 97.2%, trauma 97.8%). For THA, 5-year dislocation rates were not statistically different (nonarthroplasty/nontrauma 95.7%, arthroplasty 96.3%, trauma 96.9%), nor were five-year revision rates (nonarthroplasty/nontrauma 93.9%, arthroplasty 93.8%, trauma 95.0%). For PP, 5-year revision rates were not statistically different (nonarthroplasty/nontrauma 93.8%, arthroplasty 95.1%, trauma 95.2%).</p><p><strong>Conclusion: </strong>Femoral neck fractures were predominantly treated by nonarthroplasty/nontrauma surgeons. Nonetheless, 90-day adverse outcomes and five-year rates of revision/dislocation were clinically quite similar. This can provide confidence that those who self-select to treat geriatric femoral neck fractures are performing comparably regardless of subspecialty.</p>","PeriodicalId":45062,"journal":{"name":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","volume":"9 9","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12448162/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5435/JAAOSGlobal-D-25-00103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Geriatric femoral neck fractures are common and typically managed with hemiarthroplasty (HA), total hip arthroplasty (THA), or percutaneous pinning (PP) by an on-call physician. The current study assessed if perioperative or longer-term outcomes correlated with orthopaedic surgeon subspecialty.
Methods: The 2016 to 2022 PearlDiver M161 Ortho administrative data set was used to identify patients >65 years who underwent HA, THA, or PP for femoral neck fracture. The subspecialty of the treating surgeon was defined as arthroplasty, trauma, or nonarthroplasty/nontrauma. Exclusion criteria included polytrauma and concurrent neoplasms/infections. For each surgery type, 90-day perioperative adverse events were assessed between surgeon cohorts using multivariate logistic regression. Five-year revisions/dislocations were also assessed.
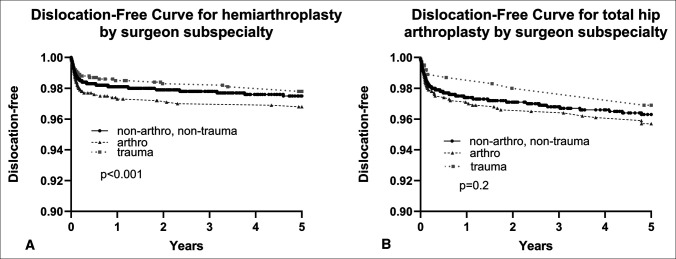
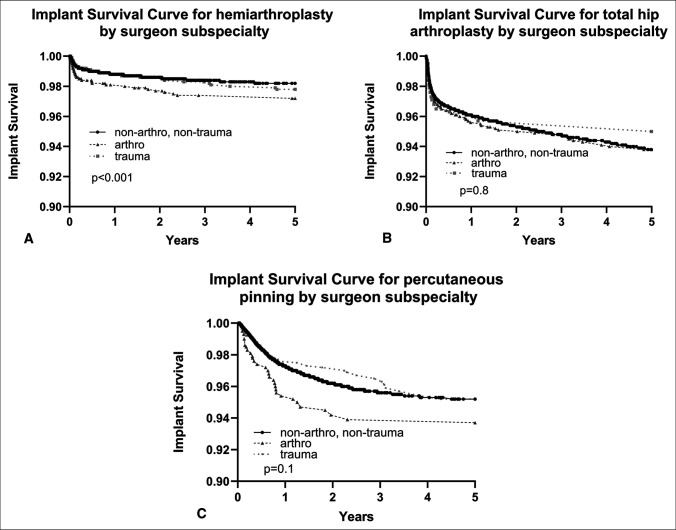
Results: Overall, 150,728 surgeries were identified (140,850 by nontrauma/nonarthroplasty surgeons, 5,013 arthroplasty, and 4,865 trauma). Arthroplasty surgeons performed THA at higher rates than trauma or nonarthroplasty/nontrauma surgeons (28.1% versus 7.7% and 12.8%, respectively, P < 0.001). Ninety-day outcomes were more similar than different across surgeon specialties. For HA, 5-year dislocation rates were statistically different but within 1% between cohorts (nonarthroplasty/nontrauma 97.5%, arthroplasty 96.8%, trauma 97.8%). Five-year revision rates were also within 1% between the cohorts (nonarthroplasty/nontrauma 98.2%, arthroplasty 97.2%, trauma 97.8%). For THA, 5-year dislocation rates were not statistically different (nonarthroplasty/nontrauma 95.7%, arthroplasty 96.3%, trauma 96.9%), nor were five-year revision rates (nonarthroplasty/nontrauma 93.9%, arthroplasty 93.8%, trauma 95.0%). For PP, 5-year revision rates were not statistically different (nonarthroplasty/nontrauma 93.8%, arthroplasty 95.1%, trauma 95.2%).
Conclusion: Femoral neck fractures were predominantly treated by nonarthroplasty/nontrauma surgeons. Nonetheless, 90-day adverse outcomes and five-year rates of revision/dislocation were clinically quite similar. This can provide confidence that those who self-select to treat geriatric femoral neck fractures are performing comparably regardless of subspecialty.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


