Development and validation of a predictive nomogram for leptomeningeal metastasis risk in NSCLC brain metastases: role of tumor location, driver mutations, and stereotactic radiosurgery.
Shoaib Bashir, Song Jian, Weiping Hong, Hui Wang, Mingyao Lai, Hanbo Lin, Qianwen Liang, Meng Xu, Linbo Cai
{"title":"Development and validation of a predictive nomogram for leptomeningeal metastasis risk in NSCLC brain metastases: role of tumor location, driver mutations, and stereotactic radiosurgery.","authors":"Shoaib Bashir, Song Jian, Weiping Hong, Hui Wang, Mingyao Lai, Hanbo Lin, Qianwen Liang, Meng Xu, Linbo Cai","doi":"10.1007/s11060-025-05220-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non-small cell lung cancer (NSCLC) frequently metastasizes to the leptomeninges, typically following brain parenchymal metastases (BM), with a significant impact on prognosis. However, predictors of leptomeningeal metastasis (LM) development remain poorly characterized. This study aimed to identify independent risk factors for subsequent LM development and establish a predictive nomogram for clinical risk stratification.</p><p><strong>Methods: </strong>The final analysis included 112 pathologically definite NSCLC patients with BM, treated at Sanjiu Brain Hospital between July 2014 and December 2020, who had not undergone whole brain radiation therapy before LM diagnosis. LM diagnosis was made if the patient had a history of pathologically confirmed lung cancer, new signs and symptoms of the nervous system, and positive CSF cytology or typical MRI findings. The data were retrospectively collected following the initial BM diagnosis until the patient was diagnosed with LM or died of any cause without developing LM. MR images were reviewed independently by two well-experienced radiologists in a double-blind manner. The primary outcome was to identify factors associated with the development of LM following BM diagnosis.</p><p><strong>Results: </strong>In the present study, two study cohorts were analyzed: (1) NSCLC-BM patients who subsequently developed LM (n = 56), and (2) NSCLC-BM patients who did not develop LM until death (n = 56). The median follow-up time for the entire cohort was 9.9 months (IQR, 4.2-18.2 months) following BM diagnosis. Univariate analysis identified several potential risk factors including EGFR/ALK/ROS1 mutations (OR = 3.868, 95% CI 1.583-10.079, P = 0.003), ventricle- or pia mater-adherent BMs (OR = 10.278, 95% CI 4.203-27.375, P < 0.001), and stereotactic radiosurgery (SRS) as a protective factor (OR = 0.024, 95% CI 0.001-0.12, P < 0.001). Multivariable logistic regression confirmed adherent BMs (OR = 9.846, 95% CI 2.981-40.176, P < 0.001) and driver mutations (OR = 5.501, 95% CI 1.444-25.893, P = 0.018) were independent predictors of increased LM risk, while SRS significantly reduced LM risk (OR = 0.029, 95% CI 0.001-0.179, P = 0.002). Fine-Gray competing risks analysis (death without developing LM as competing event) yielded consistent results: adherent BMs (HR = 3.17, 95% CI 1.68-5.97, P < 0.001), mutations (HR = 2.99, 95% CI 1.03-8.70, P = 0.045), and protective effect of SRS (HR = 0.25, 95% CI 0.14-0.46, P < 0.001). A nomogram incorporating these three factors demonstrated excellent predictive performance with an area under the receiver operating characteristic curve of 0.885 and a C-index of 0.805.</p><p><strong>Conclusions: </strong>Patients with adherent BMs and driver mutations appear to be associated with increased LM risk, while SRS may be associated with reducing this risk. Our novel nomogram incorporating these factors shows promising predictive performance in our cohort, potentially enabling effective risk stratification. These exploratory findings suggest high-risk patients with ventricle- or pia mater-adherent BMs and driver mutations might benefit from consideration of upfront SRS combined with targeted therapy, though prospective validation is needed.</p>","PeriodicalId":16425,"journal":{"name":"Journal of Neuro-Oncology","volume":" ","pages":"1377-1390"},"PeriodicalIF":3.1000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12511215/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neuro-Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11060-025-05220-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/18 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Non-small cell lung cancer (NSCLC) frequently metastasizes to the leptomeninges, typically following brain parenchymal metastases (BM), with a significant impact on prognosis. However, predictors of leptomeningeal metastasis (LM) development remain poorly characterized. This study aimed to identify independent risk factors for subsequent LM development and establish a predictive nomogram for clinical risk stratification.
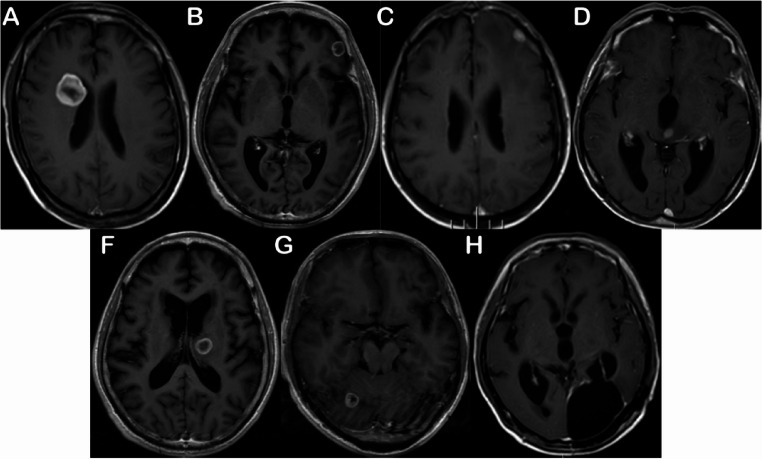
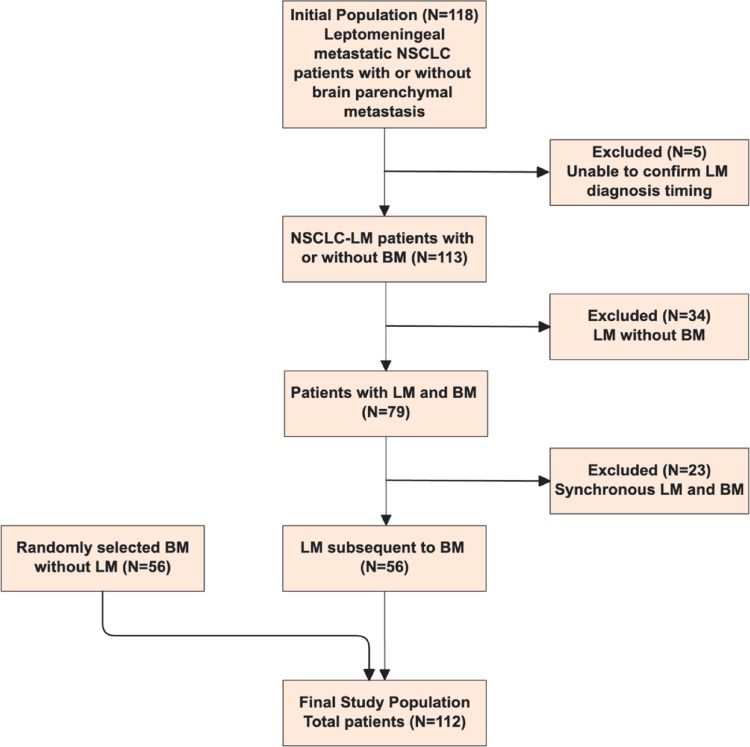
Methods: The final analysis included 112 pathologically definite NSCLC patients with BM, treated at Sanjiu Brain Hospital between July 2014 and December 2020, who had not undergone whole brain radiation therapy before LM diagnosis. LM diagnosis was made if the patient had a history of pathologically confirmed lung cancer, new signs and symptoms of the nervous system, and positive CSF cytology or typical MRI findings. The data were retrospectively collected following the initial BM diagnosis until the patient was diagnosed with LM or died of any cause without developing LM. MR images were reviewed independently by two well-experienced radiologists in a double-blind manner. The primary outcome was to identify factors associated with the development of LM following BM diagnosis.
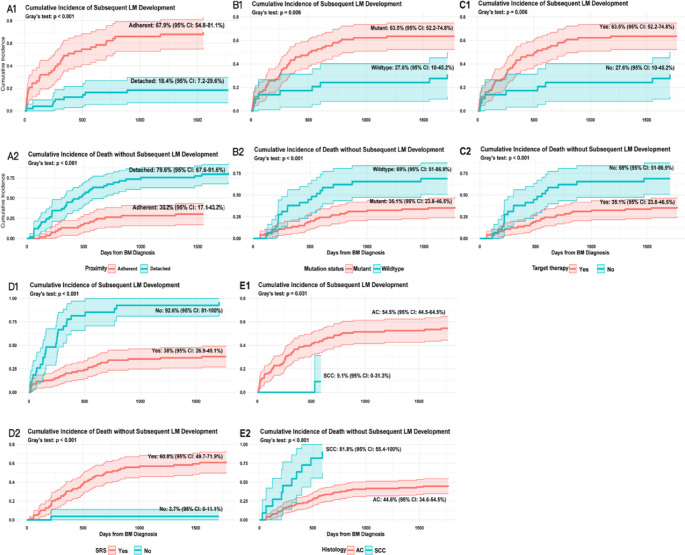
Results: In the present study, two study cohorts were analyzed: (1) NSCLC-BM patients who subsequently developed LM (n = 56), and (2) NSCLC-BM patients who did not develop LM until death (n = 56). The median follow-up time for the entire cohort was 9.9 months (IQR, 4.2-18.2 months) following BM diagnosis. Univariate analysis identified several potential risk factors including EGFR/ALK/ROS1 mutations (OR = 3.868, 95% CI 1.583-10.079, P = 0.003), ventricle- or pia mater-adherent BMs (OR = 10.278, 95% CI 4.203-27.375, P < 0.001), and stereotactic radiosurgery (SRS) as a protective factor (OR = 0.024, 95% CI 0.001-0.12, P < 0.001). Multivariable logistic regression confirmed adherent BMs (OR = 9.846, 95% CI 2.981-40.176, P < 0.001) and driver mutations (OR = 5.501, 95% CI 1.444-25.893, P = 0.018) were independent predictors of increased LM risk, while SRS significantly reduced LM risk (OR = 0.029, 95% CI 0.001-0.179, P = 0.002). Fine-Gray competing risks analysis (death without developing LM as competing event) yielded consistent results: adherent BMs (HR = 3.17, 95% CI 1.68-5.97, P < 0.001), mutations (HR = 2.99, 95% CI 1.03-8.70, P = 0.045), and protective effect of SRS (HR = 0.25, 95% CI 0.14-0.46, P < 0.001). A nomogram incorporating these three factors demonstrated excellent predictive performance with an area under the receiver operating characteristic curve of 0.885 and a C-index of 0.805.
Conclusions: Patients with adherent BMs and driver mutations appear to be associated with increased LM risk, while SRS may be associated with reducing this risk. Our novel nomogram incorporating these factors shows promising predictive performance in our cohort, potentially enabling effective risk stratification. These exploratory findings suggest high-risk patients with ventricle- or pia mater-adherent BMs and driver mutations might benefit from consideration of upfront SRS combined with targeted therapy, though prospective validation is needed.
期刊介绍:
The Journal of Neuro-Oncology is a multi-disciplinary journal encompassing basic, applied, and clinical investigations in all research areas as they relate to cancer and the central nervous system. It provides a single forum for communication among neurologists, neurosurgeons, radiotherapists, medical oncologists, neuropathologists, neurodiagnosticians, and laboratory-based oncologists conducting relevant research. The Journal of Neuro-Oncology does not seek to isolate the field, but rather to focus the efforts of many disciplines in one publication through a format which pulls together these diverse interests. More than any other field of oncology, cancer of the central nervous system requires multi-disciplinary approaches. To alleviate having to scan dozens of journals of cell biology, pathology, laboratory and clinical endeavours, JNO is a periodical in which current, high-quality, relevant research in all aspects of neuro-oncology may be found.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


