Min Fan, Joseph E Blais, Ian C K Wong, Jesse Zhao, Ka Shing Cheung, Esther W Y Chan, Angel Y S Wong, Celine S L Chui
{"title":"Risk of Ischaemic Stroke Varies With Antithrombotic Drugs Use in Proton Pump Inhibitor Users: A Self-Controlled Case Series Study.","authors":"Min Fan, Joseph E Blais, Ian C K Wong, Jesse Zhao, Ka Shing Cheung, Esther W Y Chan, Angel Y S Wong, Celine S L Chui","doi":"10.1002/pds.70219","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The conflicting findings on the association between proton pump inhibitors (PPIs) and ischaemic stroke could be due to residual confounding. Self-controlled case series (SCCS) can be used to avoid time-invariant confounding. Additionally, different baseline risks of stroke should be considered, as some individuals may be prescribed PPIs for gastroprotection from bleeding with antithrombotic drugs.</p><p><strong>Methods: </strong>We identified adult patients with incident ischaemic stroke from 2003 to 2014 in Hong Kong and applied the modified SCCS. The exposure window was pre-defined as Days 1-30, 31-60, 61-90, and 91 to the prescription end, since the PPI prescription. All other periods were referent windows. We estimated incidence rate ratios (IRR) and stratified them further using antithrombotic drugs.</p><p><strong>Results: </strong>A total of 18 170 patients were included. The IRRs for ischaemic stroke were 1.55 (95% CI: 1.00-2.42) during days 61 to 90, 1.51 (95% CI: 1.14-2.00) during days 91 to end, versus the referent window. There was no evidence of an increased risk in other risk windows versus the referent windows. In the stratified analysis, we observed an increased risk in people co-prescribed PPIs with antithrombotic drugs in all risk periods, but no increased risks among those with PPI monotherapy versus the referent window.</p><p><strong>Conclusion: </strong>No evidence of a higher ischaemic stroke after monotherapy of PPI use. The increased risk of ischaemic stroke associated with PPIs could be due to their high baseline risk prescribed with antithrombotic drugs for primary prevention. Clinical monitoring of ischaemic stroke is recommended in these people.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 9","pages":"e70219"},"PeriodicalIF":2.4000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445257/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70219","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The conflicting findings on the association between proton pump inhibitors (PPIs) and ischaemic stroke could be due to residual confounding. Self-controlled case series (SCCS) can be used to avoid time-invariant confounding. Additionally, different baseline risks of stroke should be considered, as some individuals may be prescribed PPIs for gastroprotection from bleeding with antithrombotic drugs.
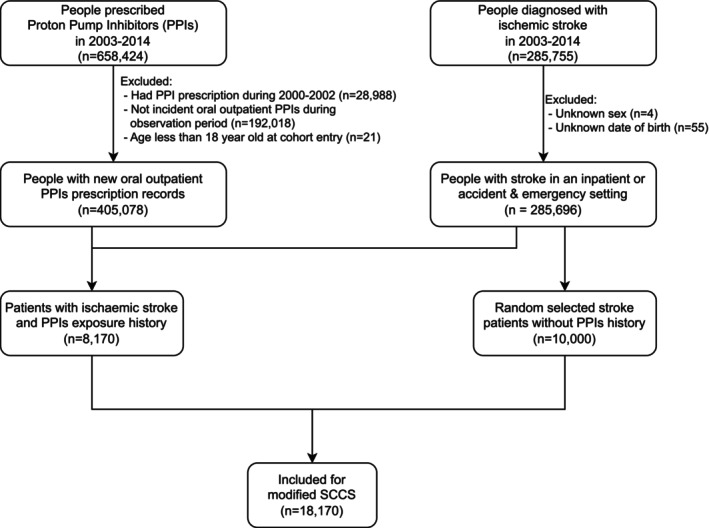
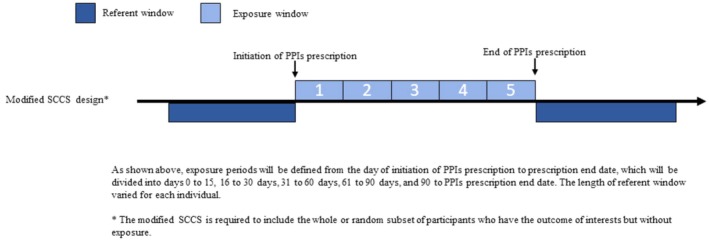
Methods: We identified adult patients with incident ischaemic stroke from 2003 to 2014 in Hong Kong and applied the modified SCCS. The exposure window was pre-defined as Days 1-30, 31-60, 61-90, and 91 to the prescription end, since the PPI prescription. All other periods were referent windows. We estimated incidence rate ratios (IRR) and stratified them further using antithrombotic drugs.
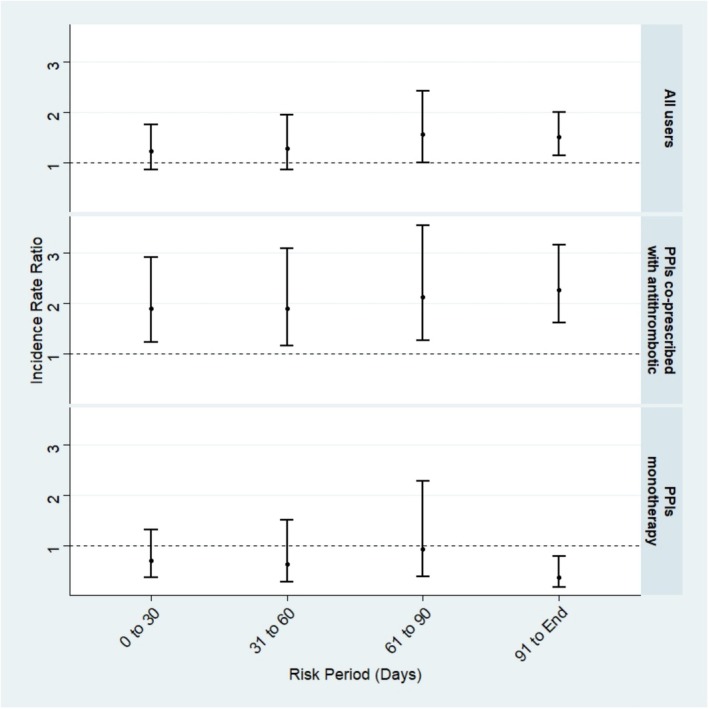
Results: A total of 18 170 patients were included. The IRRs for ischaemic stroke were 1.55 (95% CI: 1.00-2.42) during days 61 to 90, 1.51 (95% CI: 1.14-2.00) during days 91 to end, versus the referent window. There was no evidence of an increased risk in other risk windows versus the referent windows. In the stratified analysis, we observed an increased risk in people co-prescribed PPIs with antithrombotic drugs in all risk periods, but no increased risks among those with PPI monotherapy versus the referent window.
Conclusion: No evidence of a higher ischaemic stroke after monotherapy of PPI use. The increased risk of ischaemic stroke associated with PPIs could be due to their high baseline risk prescribed with antithrombotic drugs for primary prevention. Clinical monitoring of ischaemic stroke is recommended in these people.
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


