Collecting and Sharing Person-Centered AI Clinical Summaries Across Frailty Services Provided by the National Health Service and Voluntary, Community, and Social Enterprise: Protocol for a Co-Design and Feasibility Study.
Kieran Green, Sheena Asthana, Oscar Josue Ponce-Ponte, John Downey, Joanne Watson
{"title":"Collecting and Sharing Person-Centered AI Clinical Summaries Across Frailty Services Provided by the National Health Service and Voluntary, Community, and Social Enterprise: Protocol for a Co-Design and Feasibility Study.","authors":"Kieran Green, Sheena Asthana, Oscar Josue Ponce-Ponte, John Downey, Joanne Watson","doi":"10.2196/68511","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Due to its association with multimorbidity, frailty gives rise to multidimensional needs for different services. Too often, patient preferences and service encounter information are not adequately shared.</p><p><strong>Objective: </strong>This developmental study aims to co-design, collect, and analyze encounter data from multiple community and primary-based multidisciplinary teams (MDTs) providing services for people with frailty to develop prototype large language models that can generate clinical and person-centered care summaries.</p><p><strong>Methods: </strong>Engaging stakeholders in 2 primary care networks, we will co-design the large language model to ensure it meets local needs and preferences as well as infrastructure, information governance, and regulation requirements. General practitioners will identify 50 patients with frailty requiring MDT engagement. Three consecutive encounters between the patients and different members of MDTs will then be audio-recorded. Recordings will be transcribed into text for concept design and model pretraining. These data combine stakeholder engagement insights to develop sensitive artificial intelligence (AI) models responding to stakeholders' needs, workflows, and preferences. To generate the person-centered summaries, we will test 2 approaches to modeling the encounter data: graph-based modeling and hierarchical transformers. The AI-generated summaries will be compared to human-written summaries of the same encounter data and assessed for accuracy, quality, fluency, and person-centeredness. They will also be shared with the original MDT members for validation. We will capture inputs, processes, and outcomes across all key phases of the implementation journey to identify capability requirements, determinants of implementation (including key challenges and best practices to overcome them), and the value added by the technology.</p><p><strong>Results: </strong>This protocol aims to review implementation evidence and engage stakeholders in co-design. This work package will aid the development of contextually sensitive, longitudinal, and AI-generated person-centered summarization tools. Model development will aim to achieve longitudinal person-centered summaries tested against MDT standards. If deemed suitable for deployment, optimum ways of integrating these summaries into shared care records will be explored with local key system leaders. Model evaluations will provide conclusive insights into such technologies' benefits and risks. As of August 2025, this study has not yet been funded, nor has ethical approval for the project been obtained. Consequently, dates of data collection and numbers of recruited participants are not applicable at this time.</p><p><strong>Conclusions: </strong>Our protocol provides a robust method of co-designing, evaluating, and implementing a longitudinal AI medical summary tool. Including key stakeholders at multiple stages facilitates an iterative development strategy that is designed to solve implementation challenges as they emerge. This project fits within our long-term vision to deliver a multimodal AI tool that saves clinicians time and deepens the health care professional-patient relationship. Future studies should include a larger patient sample, video-recorded health care professional-patient encounters, and a more extensive longitudinal evaluation.</p><p><strong>International registered report identifier (irrid): </strong>PRR1-10.2196/68511.</p>","PeriodicalId":14755,"journal":{"name":"JMIR Research Protocols","volume":"14 ","pages":"e68511"},"PeriodicalIF":1.5000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12489409/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Research Protocols","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/68511","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Due to its association with multimorbidity, frailty gives rise to multidimensional needs for different services. Too often, patient preferences and service encounter information are not adequately shared.
Objective: This developmental study aims to co-design, collect, and analyze encounter data from multiple community and primary-based multidisciplinary teams (MDTs) providing services for people with frailty to develop prototype large language models that can generate clinical and person-centered care summaries.
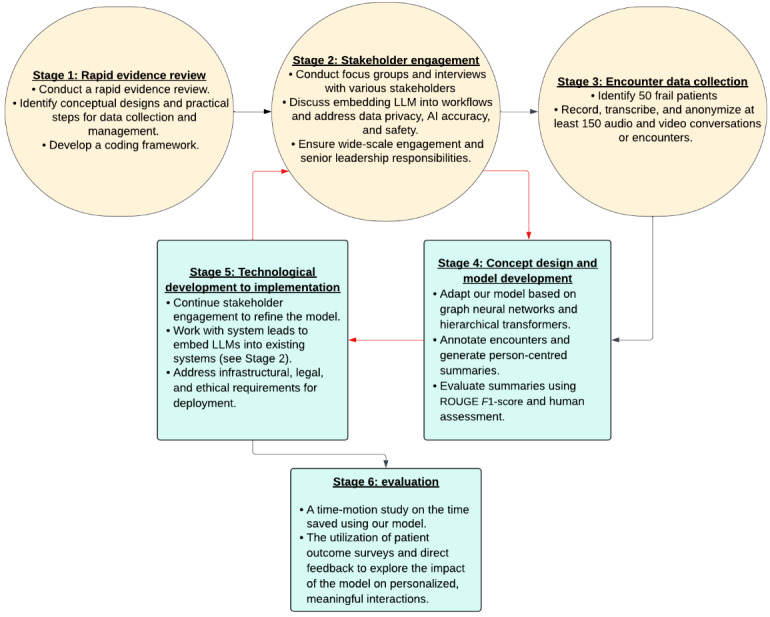
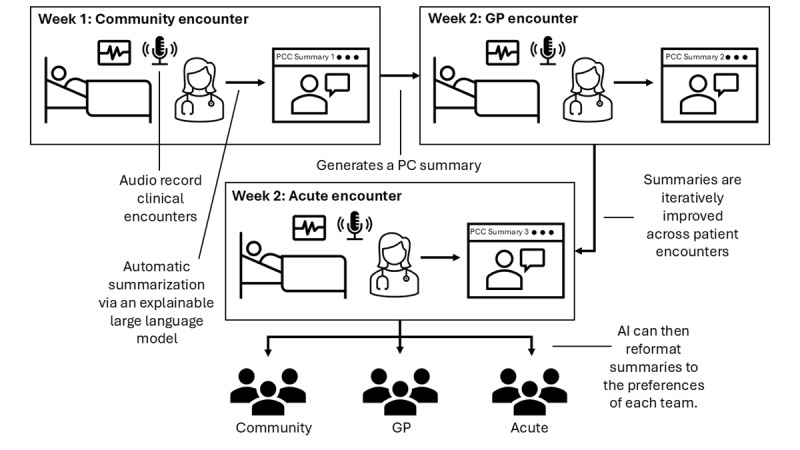
Methods: Engaging stakeholders in 2 primary care networks, we will co-design the large language model to ensure it meets local needs and preferences as well as infrastructure, information governance, and regulation requirements. General practitioners will identify 50 patients with frailty requiring MDT engagement. Three consecutive encounters between the patients and different members of MDTs will then be audio-recorded. Recordings will be transcribed into text for concept design and model pretraining. These data combine stakeholder engagement insights to develop sensitive artificial intelligence (AI) models responding to stakeholders' needs, workflows, and preferences. To generate the person-centered summaries, we will test 2 approaches to modeling the encounter data: graph-based modeling and hierarchical transformers. The AI-generated summaries will be compared to human-written summaries of the same encounter data and assessed for accuracy, quality, fluency, and person-centeredness. They will also be shared with the original MDT members for validation. We will capture inputs, processes, and outcomes across all key phases of the implementation journey to identify capability requirements, determinants of implementation (including key challenges and best practices to overcome them), and the value added by the technology.
Results: This protocol aims to review implementation evidence and engage stakeholders in co-design. This work package will aid the development of contextually sensitive, longitudinal, and AI-generated person-centered summarization tools. Model development will aim to achieve longitudinal person-centered summaries tested against MDT standards. If deemed suitable for deployment, optimum ways of integrating these summaries into shared care records will be explored with local key system leaders. Model evaluations will provide conclusive insights into such technologies' benefits and risks. As of August 2025, this study has not yet been funded, nor has ethical approval for the project been obtained. Consequently, dates of data collection and numbers of recruited participants are not applicable at this time.
Conclusions: Our protocol provides a robust method of co-designing, evaluating, and implementing a longitudinal AI medical summary tool. Including key stakeholders at multiple stages facilitates an iterative development strategy that is designed to solve implementation challenges as they emerge. This project fits within our long-term vision to deliver a multimodal AI tool that saves clinicians time and deepens the health care professional-patient relationship. Future studies should include a larger patient sample, video-recorded health care professional-patient encounters, and a more extensive longitudinal evaluation.
International registered report identifier (irrid): PRR1-10.2196/68511.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


