{"title":"Equivalent Patient-Reported Clinical Outcomes Between Single-Level and Multilevel Biportal Endoscopic Decompression at 5-Year Follow-up.","authors":"Ju Eun Kim, Eugene J Park, Daniel K Park","doi":"10.5435/JAAOSGlobal-D-24-00371","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>Retrospective.</p><p><strong>Objective: </strong>To compare long term clinical outcomes of single-level versus multilevel decompression using unilateral biportal endoscopic (UBE) decompression for degenerative lumbar spinal stenosis without instability.</p><p><strong>Summary of background data: </strong>Unilateral biportal endoscopic decompression has been shown to be effective in alleviating spinal stenosis without instability. Long-term data are lacking, and, in particular, a comparison between single-level and multilevel surgery using this minimally invasive technique has not been presented.</p><p><strong>Methods: </strong>Ninety-eight patients in each group were propensity matched based on demographics. All patients had at least 5-year follow-up. Clinical outcomes, including Oswestry Disability Index, visual analog system (VAS), time to ambulation, surgical time, and length of hospital stay, were investigated.</p><p><strong>Result: </strong>Oswestry Disability Index improved from 62.98 ± 11.53 before surgery to 18.51 ± 8.63 at the final follow-up in single-level decompression (P < 0.001). Multilevel decompression demonstrated improvement from 64.66 ± 13.71 to 19.31 ± 9.42 (P < 0.001). Similarly, leg and back VAS decreased from 7.39 ± 0.91 and 6.11 ± 1.21 before surgery to 1.72 ± 0.548 and 1.82 ± 0.67 at the last follow-up (P < 0.001) for single-level decompression. In comparison, for the multilevel, leg and back VAS improved from 7.47 ± 1.09 and 6.29 ± 1.28 to 1.86 ± 0.58 and 1.91 ± 0.75 (P < 0.001). No difference was observed between the groups at any time point. Complications and revision rates did not differ. Time to ambulation and length stay was markedly longer in multilevel.</p><p><strong>Conclusion: </strong>Outcomes, complication, and revision rates do not differ between single level and multilevel. UBE decompression can be applied to multiple levels without compromising outcomes if multiple-level decompression is deemed necessary.</p>","PeriodicalId":45062,"journal":{"name":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","volume":"9 9","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435546/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5435/JAAOSGlobal-D-24-00371","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: Retrospective.
Objective: To compare long term clinical outcomes of single-level versus multilevel decompression using unilateral biportal endoscopic (UBE) decompression for degenerative lumbar spinal stenosis without instability.
Summary of background data: Unilateral biportal endoscopic decompression has been shown to be effective in alleviating spinal stenosis without instability. Long-term data are lacking, and, in particular, a comparison between single-level and multilevel surgery using this minimally invasive technique has not been presented.
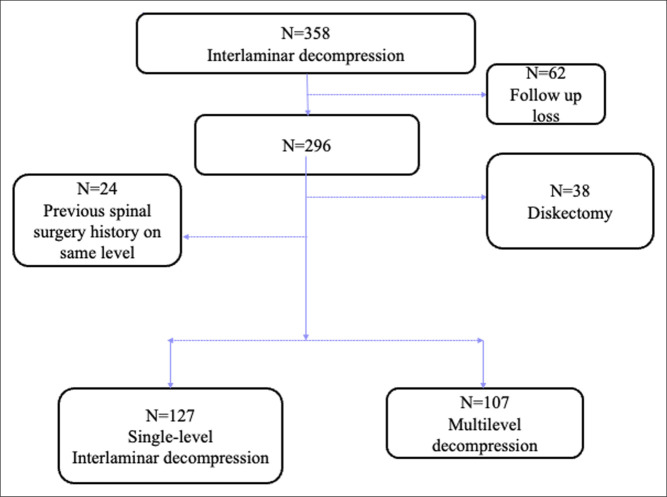
Methods: Ninety-eight patients in each group were propensity matched based on demographics. All patients had at least 5-year follow-up. Clinical outcomes, including Oswestry Disability Index, visual analog system (VAS), time to ambulation, surgical time, and length of hospital stay, were investigated.
Result: Oswestry Disability Index improved from 62.98 ± 11.53 before surgery to 18.51 ± 8.63 at the final follow-up in single-level decompression (P < 0.001). Multilevel decompression demonstrated improvement from 64.66 ± 13.71 to 19.31 ± 9.42 (P < 0.001). Similarly, leg and back VAS decreased from 7.39 ± 0.91 and 6.11 ± 1.21 before surgery to 1.72 ± 0.548 and 1.82 ± 0.67 at the last follow-up (P < 0.001) for single-level decompression. In comparison, for the multilevel, leg and back VAS improved from 7.47 ± 1.09 and 6.29 ± 1.28 to 1.86 ± 0.58 and 1.91 ± 0.75 (P < 0.001). No difference was observed between the groups at any time point. Complications and revision rates did not differ. Time to ambulation and length stay was markedly longer in multilevel.
Conclusion: Outcomes, complication, and revision rates do not differ between single level and multilevel. UBE decompression can be applied to multiple levels without compromising outcomes if multiple-level decompression is deemed necessary.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


