Shilpa Gupta, Jessica K Lee, Jerry Mitchell, Richard S P Huang
{"title":"Fibroblast Growth Factor Receptor 3 Alteration Status and Outcomes on Immune Checkpoint Inhibitors in Patients With Metastatic Urothelial Carcinoma.","authors":"Shilpa Gupta, Jessica K Lee, Jerry Mitchell, Richard S P Huang","doi":"10.1200/PO-25-00257","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The use of immune checkpoint inhibitors (ICPIs) has expanded in the treatment of metastatic urothelial carcinoma (mUC), but response rates are variable, highlighting the need for predictive biomarkers. Tumor mutational burden (TMB) has been shown to predict response to ICPI, but Fibroblast Growth Factor Receptor 3 (<i>FGFR3</i>) alterations are common drivers in mUC and there is preclinical and anecdotal evidence that they may predict less favorable outcomes to ICPIs, similar to <i>ALK</i> and <i>ROS1</i> fusions in lung cancer. We sought to explore the effect of <i>FGFR3</i> alterations alone and with TMB on response to ICPI in mUC.</p><p><strong>Methods: </strong>A total of 1,416 patients with mUC who received hybrid-capture next-generation sequencing (NGS)-based genomic profiling were evaluated for their response to ICPI and chemotherapy based on the presence of <i>FGFR3</i> alterations and TMB. A nationwide deidentified real-world clinicogenomic database (CGDB) of NGS results linked to deidentified electronic health record-derived clinical data was used to assess treatment patterns and real-world overall survival (rwOS) and real-world progression-free survival (rwPFS).</p><p><strong>Results: </strong>Among 819 patients with mUC who received ICPI, there were no significant differences in rwOS or rwPFS between <i>FGFR3</i>-altered (alt) and wild-type (wt) patients. However, among patients with TMB ≥10 mut/Mb, <i>FGFR3</i>-alt patients trended toward longer rwOS and rwPFS than <i>FGFR3</i>-wt patients. Comparing first-line ICPI versus chemotherapy and adjusting for imbalances, patients with TMB ≥10 and <i>FGFR3</i>-alt who received ICPI also trended toward longer rwPFS than patients who received chemotherapy although no significant difference in rwOS was observed.</p><p><strong>Conclusion: </strong>While <i>FGFR3</i> status alone is not predictive of response to ICPI, <i>FGFR3</i> combined with TMB emerged as a biomarker that may be predictive of response to ICPI in mUC. Further studies involving larger patient populations are warranted to confirm these findings.</p>","PeriodicalId":14797,"journal":{"name":"JCO precision oncology","volume":"9 ","pages":"e2500257"},"PeriodicalIF":5.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12442780/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCO precision oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1200/PO-25-00257","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The use of immune checkpoint inhibitors (ICPIs) has expanded in the treatment of metastatic urothelial carcinoma (mUC), but response rates are variable, highlighting the need for predictive biomarkers. Tumor mutational burden (TMB) has been shown to predict response to ICPI, but Fibroblast Growth Factor Receptor 3 (FGFR3) alterations are common drivers in mUC and there is preclinical and anecdotal evidence that they may predict less favorable outcomes to ICPIs, similar to ALK and ROS1 fusions in lung cancer. We sought to explore the effect of FGFR3 alterations alone and with TMB on response to ICPI in mUC.
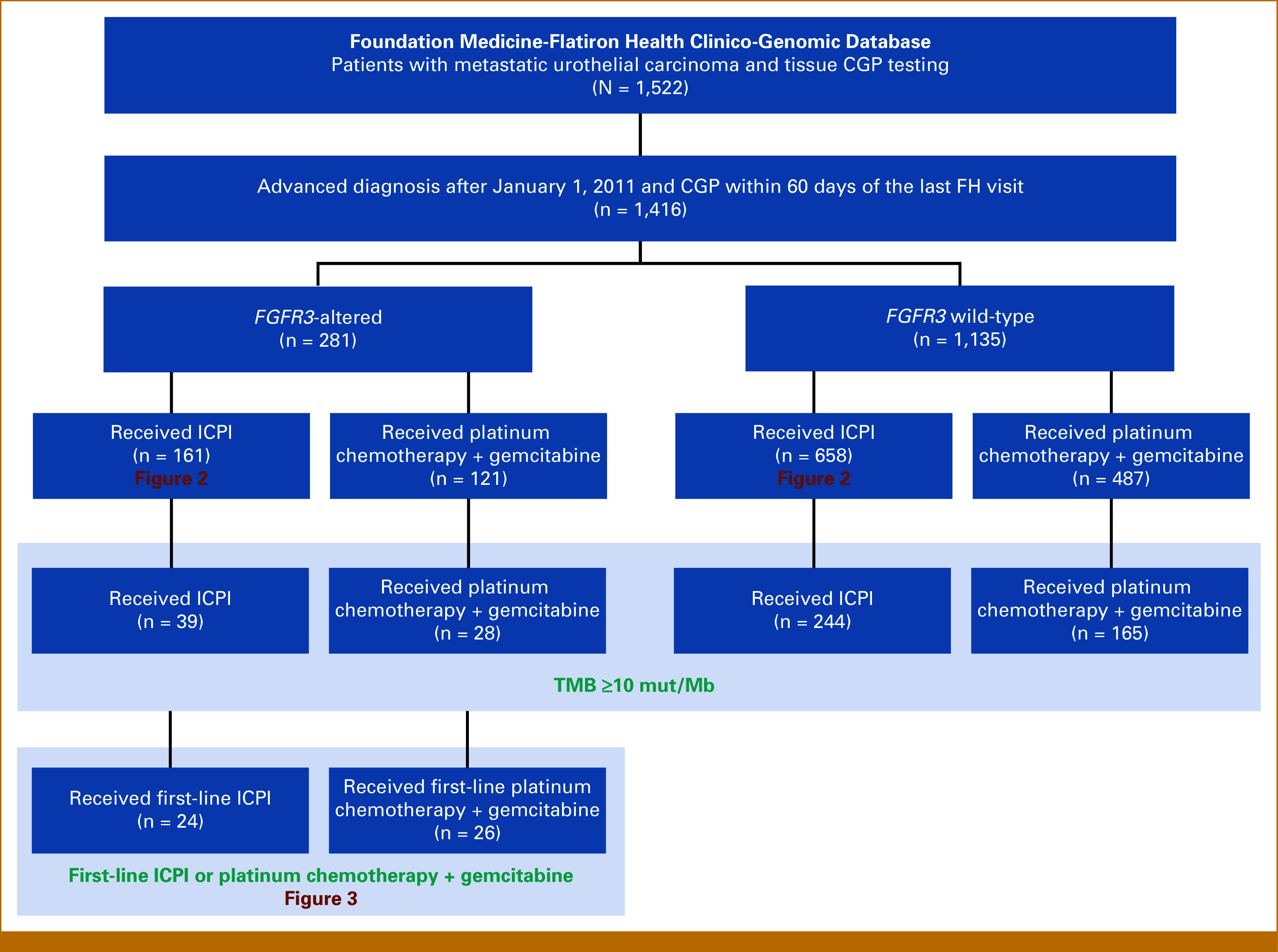
Methods: A total of 1,416 patients with mUC who received hybrid-capture next-generation sequencing (NGS)-based genomic profiling were evaluated for their response to ICPI and chemotherapy based on the presence of FGFR3 alterations and TMB. A nationwide deidentified real-world clinicogenomic database (CGDB) of NGS results linked to deidentified electronic health record-derived clinical data was used to assess treatment patterns and real-world overall survival (rwOS) and real-world progression-free survival (rwPFS).
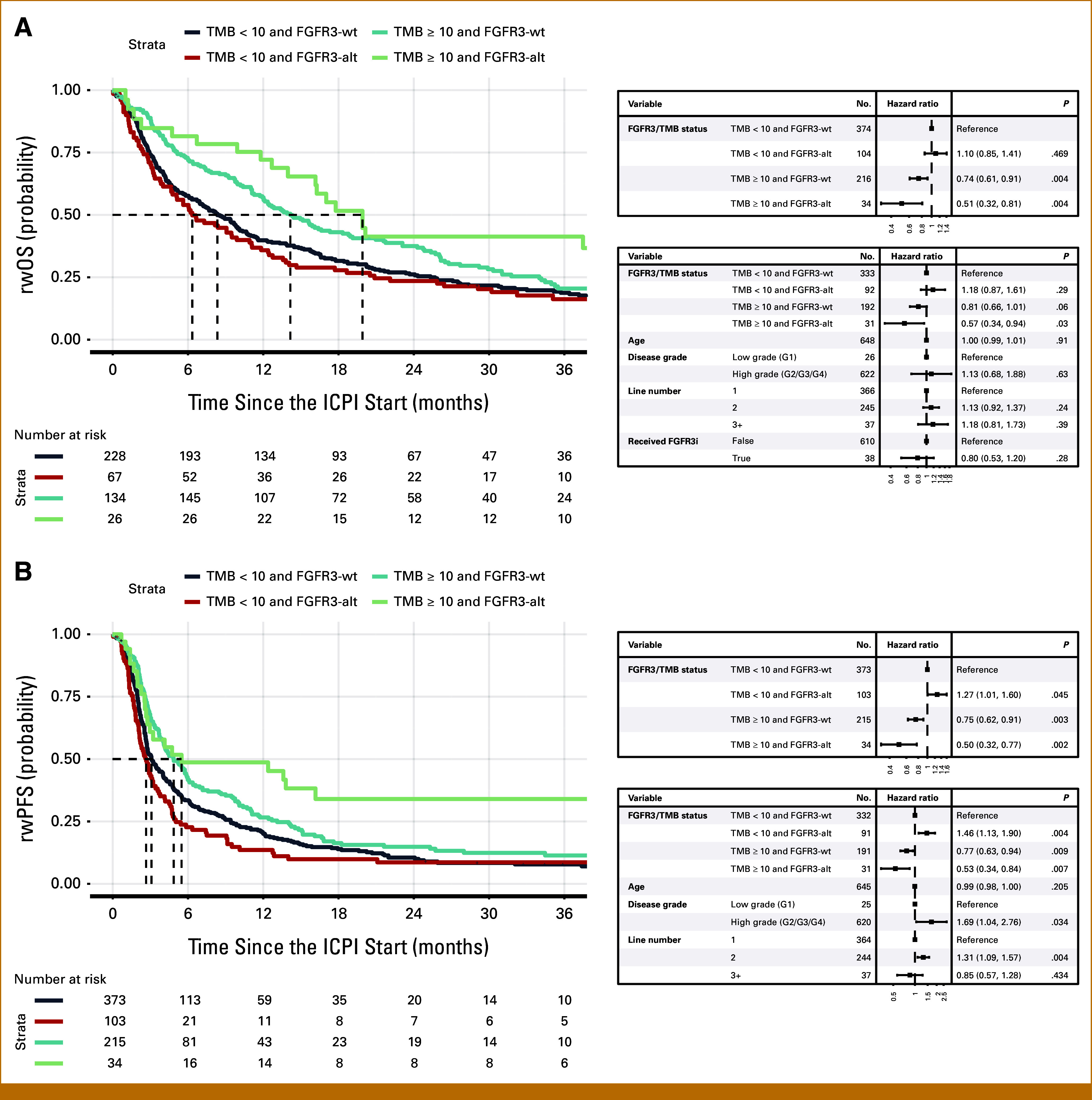
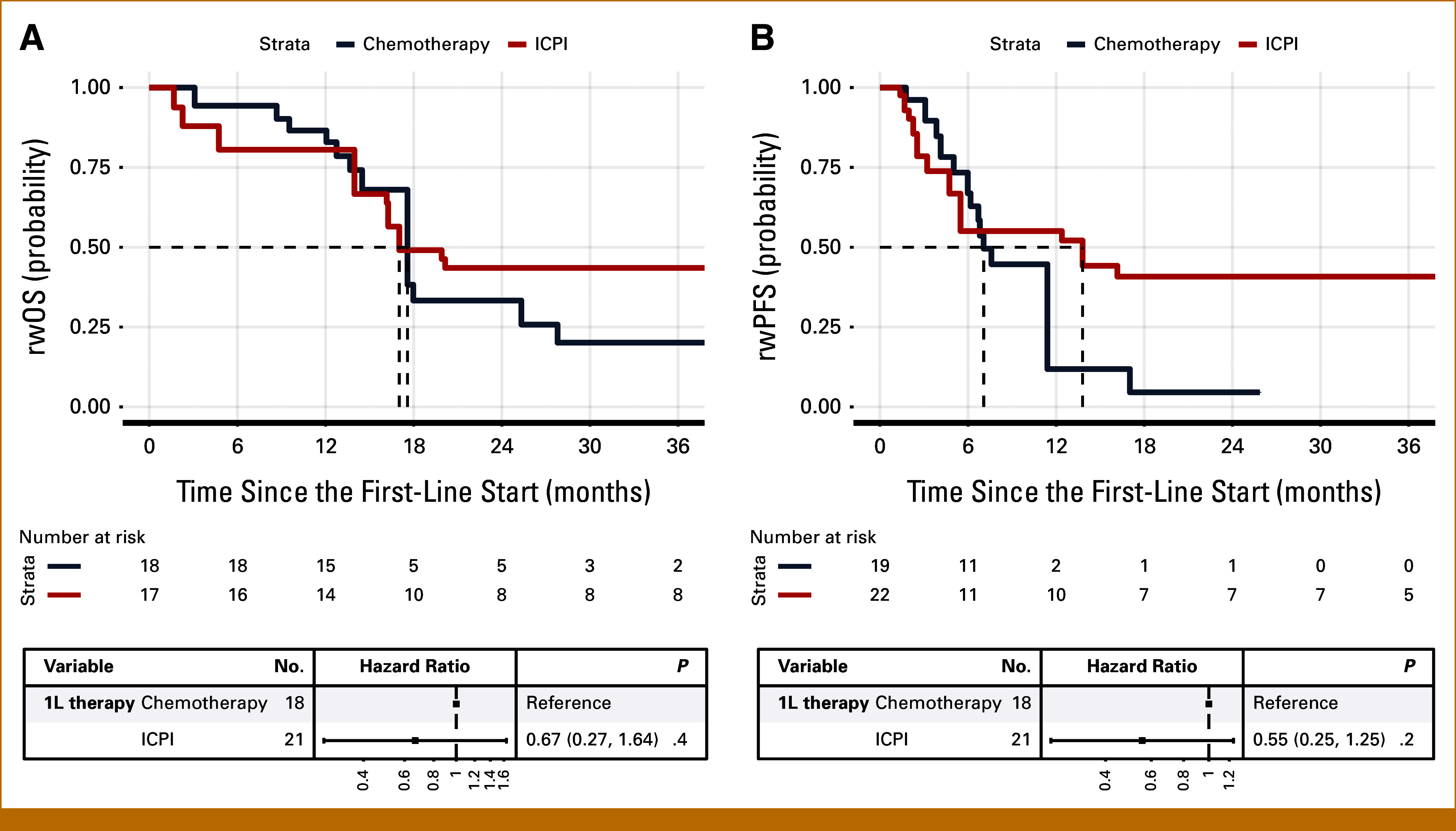
Results: Among 819 patients with mUC who received ICPI, there were no significant differences in rwOS or rwPFS between FGFR3-altered (alt) and wild-type (wt) patients. However, among patients with TMB ≥10 mut/Mb, FGFR3-alt patients trended toward longer rwOS and rwPFS than FGFR3-wt patients. Comparing first-line ICPI versus chemotherapy and adjusting for imbalances, patients with TMB ≥10 and FGFR3-alt who received ICPI also trended toward longer rwPFS than patients who received chemotherapy although no significant difference in rwOS was observed.
Conclusion: While FGFR3 status alone is not predictive of response to ICPI, FGFR3 combined with TMB emerged as a biomarker that may be predictive of response to ICPI in mUC. Further studies involving larger patient populations are warranted to confirm these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


