Incidence of diffuse parenchymal lung disease in patients meeting the Berlin definition of acute respiratory distress syndrome on mechanical ventilation.
{"title":"Incidence of diffuse parenchymal lung disease in patients meeting the Berlin definition of acute respiratory distress syndrome on mechanical ventilation.","authors":"Yasuhiro Norisue, Ryohei Yamamoto, Hideki Yamakawa, Makoto Hibino, Tatsuya Nagai, Yutaro Fujimoto, Jun Kataoka, Kenji Ishii, Takashi Hongo, Daisuke Kasugai, Yudai Iwasaki, Masaaki Sakuraya, Goji Shimizu, Tomoyuki Masuyama, Shigeki Fujitani, Yasuharu Tokuda, Takashi Ogura","doi":"10.1183/23120541.01296-2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The simplicity of the diagnostic definition of acute respiratory distress syndrome (ARDS) has led to its diagnosis in patients with new-onset or exacerbation of diffuse parenchymal lung diseases (DPLDs). This study investigated the incidence of DPLDs in patients with acute hypoxic respiratory failure who met the Berlin definition.</p><p><strong>Methods: </strong>This Japan-based multicentre retrospective cohort study included patients on mechanical ventilation who met the Berlin definition. For all participants, diagnosis was made by pulmonology specialists in DPLD and thoracic radiology (blinded to clinical diagnoses) by reviewing an extensive database designed for DPLD diagnosis across 10 participating hospitals.</p><p><strong>Results: </strong>Of 13 612 patients admitted to the intensive care unit during the study period, 272 met the Berlin definition of ARDS and were included for analysis. All underwent at least one chest computed tomography scan; none underwent lung biopsy. Briefly, 182 were designated classic ARDS (67%), 69 non-IPF (idiopathic pulmonary fibrosis) DPLDs (25%) and 21 IPF (8%) by DPLD specialists. Of the 90 patients diagnosed with DPLD (IPF or non-IPF) by specialists, 35% were diagnosed with classic ARDS by intensivists at the end of the clinical course. Diagnostic classifications of classic ARDS and IPF by DPLD specialists were associated with time-to-death (adjusted hazard ratio (HR) 1.58 (95% CI 1.03-2.45), p=0.038, and adjusted HR 1.73 (95% CI 1.01-2.97), p=0.045, respectively) and in-hospital mortality (adjusted HR 1.54 (95% CI 1.06-2.23), p=0.022 for classic ARDS) <i>versus</i> non-IPF DPLDs; intensivist diagnostic classifications were not.</p><p><strong>Conclusion: </strong>Approximately one-third of patients within the Berlin definition were retrospectively diagnosed with new-onset or acutely exacerbated DPLD by specialists.</p>","PeriodicalId":11739,"journal":{"name":"ERJ Open Research","volume":"11 5","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12434489/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ERJ Open Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1183/23120541.01296-2024","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The simplicity of the diagnostic definition of acute respiratory distress syndrome (ARDS) has led to its diagnosis in patients with new-onset or exacerbation of diffuse parenchymal lung diseases (DPLDs). This study investigated the incidence of DPLDs in patients with acute hypoxic respiratory failure who met the Berlin definition.
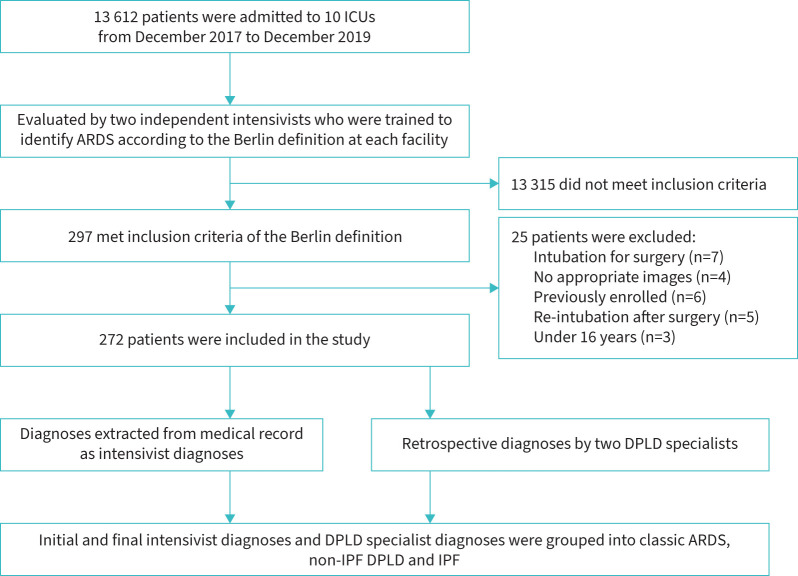
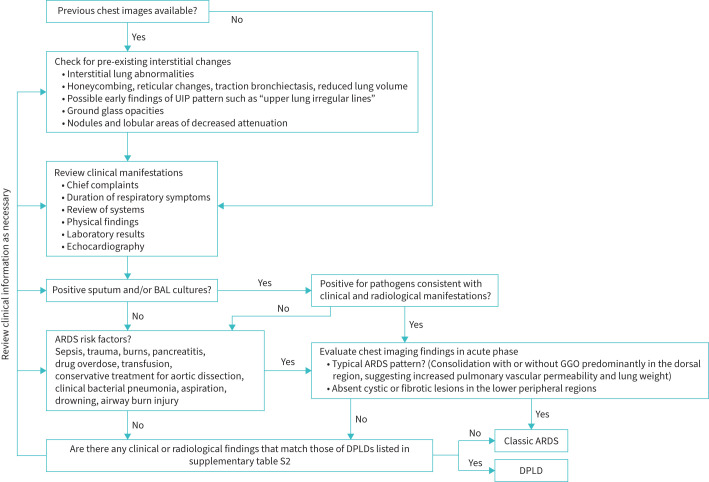
Methods: This Japan-based multicentre retrospective cohort study included patients on mechanical ventilation who met the Berlin definition. For all participants, diagnosis was made by pulmonology specialists in DPLD and thoracic radiology (blinded to clinical diagnoses) by reviewing an extensive database designed for DPLD diagnosis across 10 participating hospitals.
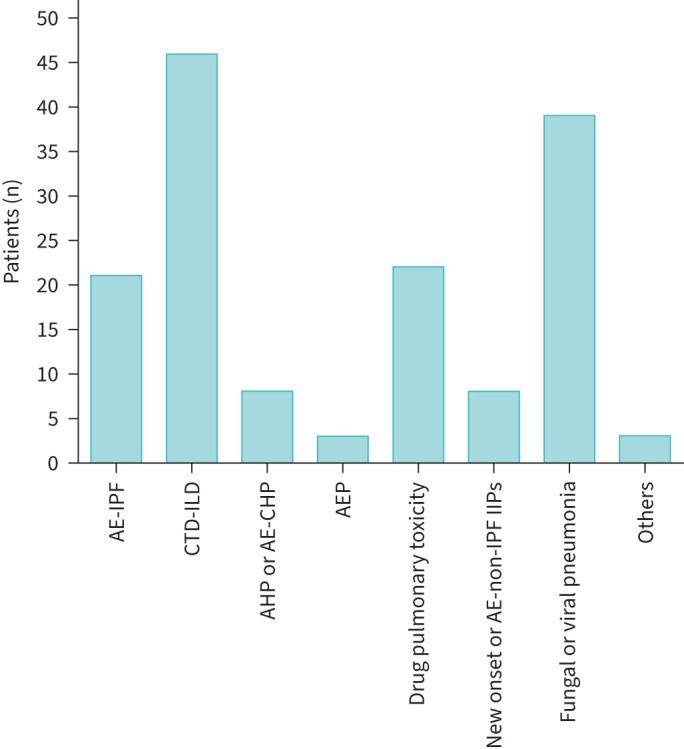
Results: Of 13 612 patients admitted to the intensive care unit during the study period, 272 met the Berlin definition of ARDS and were included for analysis. All underwent at least one chest computed tomography scan; none underwent lung biopsy. Briefly, 182 were designated classic ARDS (67%), 69 non-IPF (idiopathic pulmonary fibrosis) DPLDs (25%) and 21 IPF (8%) by DPLD specialists. Of the 90 patients diagnosed with DPLD (IPF or non-IPF) by specialists, 35% were diagnosed with classic ARDS by intensivists at the end of the clinical course. Diagnostic classifications of classic ARDS and IPF by DPLD specialists were associated with time-to-death (adjusted hazard ratio (HR) 1.58 (95% CI 1.03-2.45), p=0.038, and adjusted HR 1.73 (95% CI 1.01-2.97), p=0.045, respectively) and in-hospital mortality (adjusted HR 1.54 (95% CI 1.06-2.23), p=0.022 for classic ARDS) versus non-IPF DPLDs; intensivist diagnostic classifications were not.
Conclusion: Approximately one-third of patients within the Berlin definition were retrospectively diagnosed with new-onset or acutely exacerbated DPLD by specialists.
期刊介绍:
ERJ Open Research is a fully open access original research journal, published online by the European Respiratory Society. The journal aims to publish high-quality work in all fields of respiratory science and medicine, covering basic science, clinical translational science and clinical medicine. The journal was created to help fulfil the ERS objective to disseminate scientific and educational material to its members and to the medical community, but also to provide researchers with an affordable open access specialty journal in which to publish their work.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


