Long-term in-hospital mortality and chronic thromboembolic pulmonary hypertension after COVID-19-associated pulmonary embolism in France: a nationwide study.
Pierre Tankéré, Emilie Lajeune, Anne-Sophie Mariet, Jonathan Cottenet, Guillaume Beltramo, Marjolaine Georges, Philippe Bonniaud, Nicolas Favrolt, Catherine Quantin
{"title":"Long-term in-hospital mortality and chronic thromboembolic pulmonary hypertension after COVID-19-associated pulmonary embolism in France: a nationwide study.","authors":"Pierre Tankéré, Emilie Lajeune, Anne-Sophie Mariet, Jonathan Cottenet, Guillaume Beltramo, Marjolaine Georges, Philippe Bonniaud, Nicolas Favrolt, Catherine Quantin","doi":"10.1183/23120541.01387-2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although long-term effects of coronavirus disease-2019 (COVID-19) such as dyspnoea are frequent, the mechanisms are often poorly understood. The endothelial effects of COVID-19, such as venous or arterial thrombosis, are also well documented. Thus, the incidence of chronic thromboembolic pulmonary hypertension (CTEPH) following COVID-19 is an issue with many implications, particularly for screening in patients with long COVID.</p><p><strong>Methods: </strong>From the French National Hospital Discharge database (March 2020 to December 2021), we included all adults hospitalised for pulmonary embolism (PE). To study the hospital incidence of CTEPH, we excluded patients with previous pulmonary hypertension diagnoses. Then, in the 2 years following the admission for PE, we compared the hospital incidence of CTEPH between PE patients with COVID-19 (COVID-PE) and without (non-COVID-PE). We also studied in-hospital mortality.</p><p><strong>Results: </strong>Among the 136 505 patients included, 1.68% were diagnosed with CTEPH in the following 2 years with a significant difference between COVID-PE and non-COVID-PE (0.77% <i>versus</i> 1.82%; p<0.0001). The 2-year in-hospital mortality was significantly lower in COVID-PE than in non-COVID-PE (4.82% <i>versus</i> 13.34%; p<0.0001). These results were confirmed by multivariate analyses. Among COVID-PE, we found no difference in the hospital incidence of CTEPH between 2020 and 2021, while after the initial discharge, in-hospital mortality was significantly higher in 2020 compared with 2021.</p><p><strong>Conclusion: </strong>When investigating chronic dyspnoea in patients hospitalised for COVID-19 associated with PE, the risk of CTEPH should not be considered higher than for other PE. COVID-19 associated with hospitalised PE should not be considered an additional harmful factor if not associated with initial in-hospital mortality.</p>","PeriodicalId":11739,"journal":{"name":"ERJ Open Research","volume":"11 5","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12434486/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ERJ Open Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1183/23120541.01387-2024","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although long-term effects of coronavirus disease-2019 (COVID-19) such as dyspnoea are frequent, the mechanisms are often poorly understood. The endothelial effects of COVID-19, such as venous or arterial thrombosis, are also well documented. Thus, the incidence of chronic thromboembolic pulmonary hypertension (CTEPH) following COVID-19 is an issue with many implications, particularly for screening in patients with long COVID.
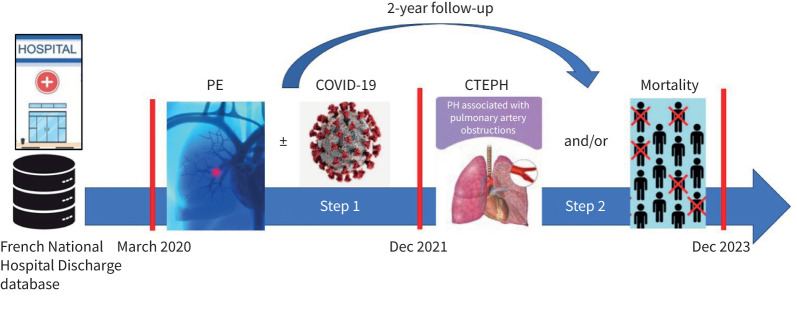
Methods: From the French National Hospital Discharge database (March 2020 to December 2021), we included all adults hospitalised for pulmonary embolism (PE). To study the hospital incidence of CTEPH, we excluded patients with previous pulmonary hypertension diagnoses. Then, in the 2 years following the admission for PE, we compared the hospital incidence of CTEPH between PE patients with COVID-19 (COVID-PE) and without (non-COVID-PE). We also studied in-hospital mortality.
Results: Among the 136 505 patients included, 1.68% were diagnosed with CTEPH in the following 2 years with a significant difference between COVID-PE and non-COVID-PE (0.77% versus 1.82%; p<0.0001). The 2-year in-hospital mortality was significantly lower in COVID-PE than in non-COVID-PE (4.82% versus 13.34%; p<0.0001). These results were confirmed by multivariate analyses. Among COVID-PE, we found no difference in the hospital incidence of CTEPH between 2020 and 2021, while after the initial discharge, in-hospital mortality was significantly higher in 2020 compared with 2021.
Conclusion: When investigating chronic dyspnoea in patients hospitalised for COVID-19 associated with PE, the risk of CTEPH should not be considered higher than for other PE. COVID-19 associated with hospitalised PE should not be considered an additional harmful factor if not associated with initial in-hospital mortality.
期刊介绍:
ERJ Open Research is a fully open access original research journal, published online by the European Respiratory Society. The journal aims to publish high-quality work in all fields of respiratory science and medicine, covering basic science, clinical translational science and clinical medicine. The journal was created to help fulfil the ERS objective to disseminate scientific and educational material to its members and to the medical community, but also to provide researchers with an affordable open access specialty journal in which to publish their work.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


