Asaad G Beshish, Rebecca Shamah, Joshua Qian, Kasey Keane-Lerner, Paola Rodriguez Morales, Tawanda Zinyandu, Joel Davis, Joshua M Rosenblum, Heather K Viamonte
{"title":"Is hyperoxia during veno-arterial extracorporeal life support due to cardiopulmonary failure associated with mortality in pediatric patients?","authors":"Asaad G Beshish, Rebecca Shamah, Joshua Qian, Kasey Keane-Lerner, Paola Rodriguez Morales, Tawanda Zinyandu, Joel Davis, Joshua M Rosenblum, Heather K Viamonte","doi":"10.1051/ject/2025006","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Data is limited regarding the effects of supraphysiologic blood oxygen tension in patients requiring extracorporeal life support (ECLS). We sought to evaluate the association between hyperoxia and outcomes in pediatric patients requiring veno-arterial (VA) ECLS.</p><p><strong>Methods: </strong>Retrospective single-center study at an academic children's hospital that included all patients 0-18 years who required VA-ECLS between 01/2014 and 12/2019.</p><p><strong>Results: </strong>During the study period, 229 VA-ECLS runs occurred in 229 patients. The majority of patients were neonates (73.4%), with cardiac being the most common indication (48.9%). The median time from admission to cannulation was 78.5 h (IQR 14, 356) with a median ECLS duration of 111.5 h (IQR 65.5, 184.5). The overall mortality rate was 44.5%. Using a receiver operating curve, a mean PaO<sub>2</sub> of 233 mmHg in the first 48 h of ECLS was determined to have the optimal discriminatory ability for mortality (sensitivity 36% and specificity 76%). Of the VA-ECLS cohort, 68 (29.7%) had a mean PaO<sub>2</sub> > 233 mmHg (hyperoxia group). The hyperoxia group tended to be older (median age 4.6 vs 1.5 months, p = 0.019), had a primary cardiac indication for VA-ECLS (60% vs 44%, p = 0.0004), and had a higher mortality rate (54% vs 40%, p = 0.050). In the multivariable analysis, after adjusting for covariables, the data demonstrated increased odds of mortality (aOR 2.02, 95% CI [1.03, 3.97], p = 0.03). The odds of development of stage II or III acute kidney injury (AKI) (aOR 2.04, 95% CI [0.82, 5.50]), but that did not reach statistical significance (p = 0.120).</p><p><strong>Conclusion: </strong>There is evidence that hyperoxia during the first 48 h of VA-ECLS may be associated with mortality and development of acute kidney injury, although this did not reach statistical significance. Multicenter and prospective evaluation of this modifiable risk factor is imperative to improve the care of this high-risk cohort.</p>","PeriodicalId":519952,"journal":{"name":"The journal of extra-corporeal technology","volume":"57 3","pages":"129-136"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435806/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The journal of extra-corporeal technology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1051/ject/2025006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Data is limited regarding the effects of supraphysiologic blood oxygen tension in patients requiring extracorporeal life support (ECLS). We sought to evaluate the association between hyperoxia and outcomes in pediatric patients requiring veno-arterial (VA) ECLS.
Methods: Retrospective single-center study at an academic children's hospital that included all patients 0-18 years who required VA-ECLS between 01/2014 and 12/2019.
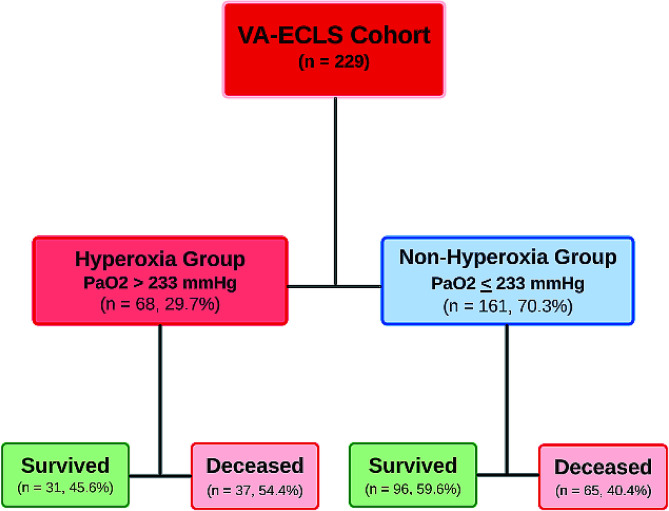
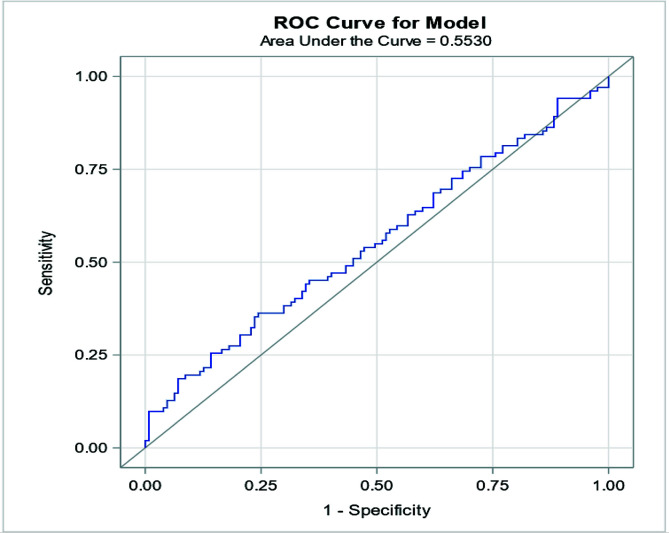
Results: During the study period, 229 VA-ECLS runs occurred in 229 patients. The majority of patients were neonates (73.4%), with cardiac being the most common indication (48.9%). The median time from admission to cannulation was 78.5 h (IQR 14, 356) with a median ECLS duration of 111.5 h (IQR 65.5, 184.5). The overall mortality rate was 44.5%. Using a receiver operating curve, a mean PaO2 of 233 mmHg in the first 48 h of ECLS was determined to have the optimal discriminatory ability for mortality (sensitivity 36% and specificity 76%). Of the VA-ECLS cohort, 68 (29.7%) had a mean PaO2 > 233 mmHg (hyperoxia group). The hyperoxia group tended to be older (median age 4.6 vs 1.5 months, p = 0.019), had a primary cardiac indication for VA-ECLS (60% vs 44%, p = 0.0004), and had a higher mortality rate (54% vs 40%, p = 0.050). In the multivariable analysis, after adjusting for covariables, the data demonstrated increased odds of mortality (aOR 2.02, 95% CI [1.03, 3.97], p = 0.03). The odds of development of stage II or III acute kidney injury (AKI) (aOR 2.04, 95% CI [0.82, 5.50]), but that did not reach statistical significance (p = 0.120).
Conclusion: There is evidence that hyperoxia during the first 48 h of VA-ECLS may be associated with mortality and development of acute kidney injury, although this did not reach statistical significance. Multicenter and prospective evaluation of this modifiable risk factor is imperative to improve the care of this high-risk cohort.
背景:关于超生理血氧张力对需要体外生命支持(ECLS)的患者的影响的数据有限。我们试图评估高氧与需要静脉-动脉(VA) ECLS的儿科患者预后之间的关系。方法:回顾性单中心研究,纳入2014年1月至2019年12月期间所有0-18岁需要VA-ECLS的患者。结果:在研究期间,229例患者发生229例VA-ECLS。大多数患者是新生儿(73.4%),心脏是最常见的适应症(48.9%)。入院至插管的中位时间为78.5 h (IQR 14, 356),中位ECLS持续时间为111.5 h (IQR 65.5, 184.5)。总死亡率为44.5%。使用受试者工作曲线,确定ECLS前48小时平均PaO2为233 mmHg具有最佳的死亡率判别能力(敏感性36%,特异性76%)。在VA-ECLS队列中,68例(29.7%)患者的平均PaO2水平为233mmhg(高氧组)。高氧组倾向于年龄较大(中位年龄4.6 vs 1.5个月,p = 0.019),具有VA-ECLS的主要心脏指征(60% vs 44%, p = 0.0004),死亡率较高(54% vs 40%, p = 0.050)。在多变量分析中,调整协变量后,数据显示死亡率增加(aOR 2.02, 95% CI [1.03, 3.97], p = 0.03)。II期或III期急性肾损伤(AKI)发生的几率(aOR 2.04, 95% CI[0.82, 5.50]),但差异无统计学意义(p = 0.120)。结论:有证据表明,VA-ECLS前48小时的高氧可能与死亡率和急性肾损伤的发展有关,尽管这没有达到统计学意义。对这一可改变的危险因素进行多中心和前瞻性评估对于改善这一高危人群的护理是必要的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


