James R Neal, Pavel V Mishin, Caitlin L Blau, Devon O Aganga, Troy G Seelhammer
{"title":"Using an intermittent flow (\"clamp and flash\") method to assess the readiness to wean from VA ECMO in adult and pediatric patients.","authors":"James R Neal, Pavel V Mishin, Caitlin L Blau, Devon O Aganga, Troy G Seelhammer","doi":"10.1051/ject/2025018","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of VA extracorporeal membrane oxygenation (ECMO) for cardiac recovery is widely adopted, with extensive publications on assessing readiness to wean from VA ECMO. Techniques to reduce ECMO support vary, including reducing flows to a low continuous cardiac index, adding bridges, temporary flow cessation, or decreasing ECMO RPMs.</p><p><strong>Method: </strong>We propose an alternative method involving repeated cycles of 3-4 min of ECMO flow cessation (\"clamp\") followed by a 30-second return (\"flash\") of flow. This method requires additional anticoagulation to achieve an elevated ACT, targeting 220 s for adults and 210 s for pediatrics with heparin drip and bolus, or 240 s for adults and 225 s for pediatrics with bivalirudin drip and heparin bolus. During the clamp period, flow is stopped in adult ECMO circuits with a single venous line clamp, while in pediatric circuits, flow continues via the manifold shunt but is stopped in the arterial and venous lines with a single venous line clamp. Flashing the circuit resumes patient flow for 30 s to circulate stagnant blood.</p><p><strong>Results: </strong>This method significantly reduces support during the trial, which lasts one hour for adults and up to two hours for pediatric patients. The heart is unsupported 85-90% of the time, with an 85% decrease in cardiac support compared to low-flow trials.</p><p><strong>Conclusion: </strong>Since 2011, our center has used this technique without thrombotic complications when the protocol is followed. Most patients removed from ECMO did not require reinstitution, with rare cases needing VV support or VA support due to sepsis onset.</p>","PeriodicalId":519952,"journal":{"name":"The journal of extra-corporeal technology","volume":"57 3","pages":"147-152"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435822/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The journal of extra-corporeal technology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1051/ject/2025018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The use of VA extracorporeal membrane oxygenation (ECMO) for cardiac recovery is widely adopted, with extensive publications on assessing readiness to wean from VA ECMO. Techniques to reduce ECMO support vary, including reducing flows to a low continuous cardiac index, adding bridges, temporary flow cessation, or decreasing ECMO RPMs.
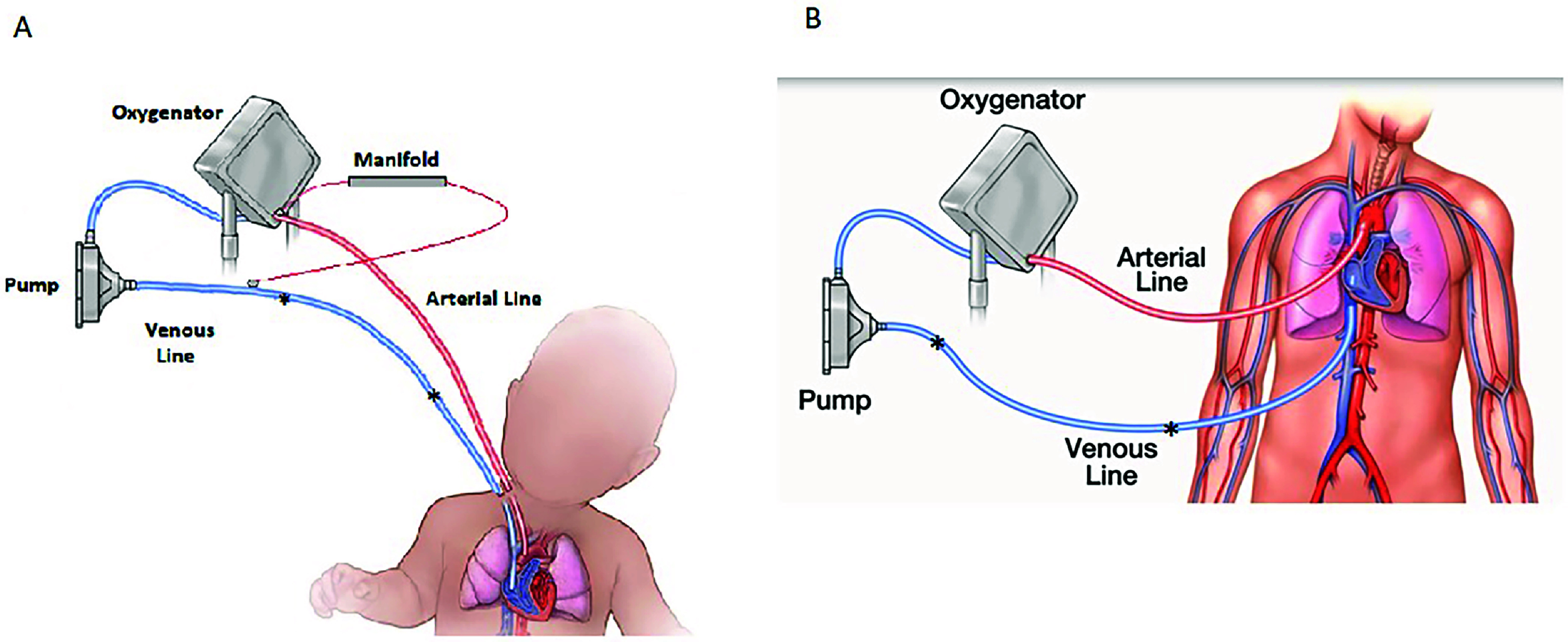
Method: We propose an alternative method involving repeated cycles of 3-4 min of ECMO flow cessation ("clamp") followed by a 30-second return ("flash") of flow. This method requires additional anticoagulation to achieve an elevated ACT, targeting 220 s for adults and 210 s for pediatrics with heparin drip and bolus, or 240 s for adults and 225 s for pediatrics with bivalirudin drip and heparin bolus. During the clamp period, flow is stopped in adult ECMO circuits with a single venous line clamp, while in pediatric circuits, flow continues via the manifold shunt but is stopped in the arterial and venous lines with a single venous line clamp. Flashing the circuit resumes patient flow for 30 s to circulate stagnant blood.
Results: This method significantly reduces support during the trial, which lasts one hour for adults and up to two hours for pediatric patients. The heart is unsupported 85-90% of the time, with an 85% decrease in cardiac support compared to low-flow trials.
Conclusion: Since 2011, our center has used this technique without thrombotic complications when the protocol is followed. Most patients removed from ECMO did not require reinstitution, with rare cases needing VV support or VA support due to sepsis onset.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


