{"title":"Amyotrophic Lateral Sclerosis Masquerading as Multiple System Atrophy with Parkinsonism and Anxiety as Initial Manifestations.","authors":"Haiyan Tang, Jianping Yao, Zhuang Wang","doi":"10.2147/DNND.S531647","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Amyotrophic lateral sclerosis (ALS) and multiple system atrophy (MSA) are both neurodegenerative disorders. While ALS may present with clinical features resembling Parkinsonism, there have been no definitive reports of ALS mimicking MSA, only cases of Primary lateral sclerosis (PLS) mimicking Parkinsonism.</p><p><strong>Methods: </strong>This article reports a case of ALS presenting with Parkinsonism and anxiety as the initial symptoms. Five years after the initial diagnosis of MSA, the patient developed signs of lower motor neuron involvement, including fasciculations and muscle atrophy, ultimately leading to a revised diagnosis of ALS. This study combines literature analysis to explore the reasons for misdiagnosis and identifies key differentiating features.</p><p><strong>Results: </strong>Specifically, muscle rigidity in ALS is characterized by a velocity-dependent increase in muscle tone caused by damage to the upper motor neurons. This symptom tends to be more pronounced in the lower limbs than in the upper limbs and is often accompanied by spastic gait. Objective examinations may reveal early atrophy of the frontal and temporal lobes of the cerebrum on head magnetic resonance (MR) imaging, whereas <sup>18</sup>F-FDG brain positron emission tomography (PET) may reveal reduced metabolism in the frontal and parietal lobes of the cerebrum with normal basal ganglial function, distinguishing ALS from basal ganglial metabolic decline in MSA.</p><p><strong>Discussion: </strong>To our knowledge, this is the first case of ALS misdiagnosed as MSA. Clinically, patients with parkinsonism who do not respond to dopaminergic drugs should be cautious about atypical ALS. Muscle rigidity manifesting as upper motor neuron damage, and MR and <sup>18</sup>F-FDG brain PET imaging can provide early differential diagnosis indicators.</p>","PeriodicalId":93972,"journal":{"name":"Degenerative neurological and neuromuscular disease","volume":"15 ","pages":"95-100"},"PeriodicalIF":3.2000,"publicationDate":"2025-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433637/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Degenerative neurological and neuromuscular disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/DNND.S531647","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Amyotrophic lateral sclerosis (ALS) and multiple system atrophy (MSA) are both neurodegenerative disorders. While ALS may present with clinical features resembling Parkinsonism, there have been no definitive reports of ALS mimicking MSA, only cases of Primary lateral sclerosis (PLS) mimicking Parkinsonism.
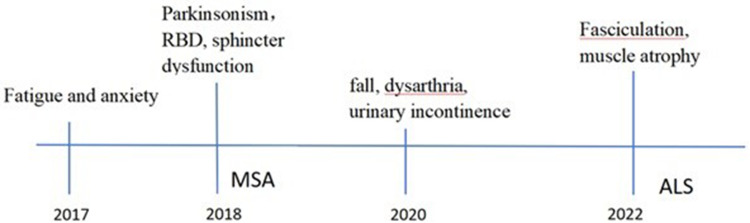
Methods: This article reports a case of ALS presenting with Parkinsonism and anxiety as the initial symptoms. Five years after the initial diagnosis of MSA, the patient developed signs of lower motor neuron involvement, including fasciculations and muscle atrophy, ultimately leading to a revised diagnosis of ALS. This study combines literature analysis to explore the reasons for misdiagnosis and identifies key differentiating features.
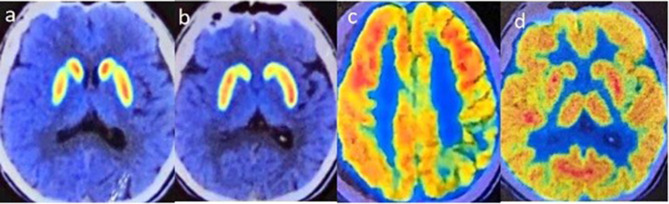
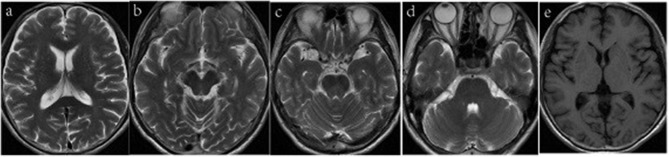
Results: Specifically, muscle rigidity in ALS is characterized by a velocity-dependent increase in muscle tone caused by damage to the upper motor neurons. This symptom tends to be more pronounced in the lower limbs than in the upper limbs and is often accompanied by spastic gait. Objective examinations may reveal early atrophy of the frontal and temporal lobes of the cerebrum on head magnetic resonance (MR) imaging, whereas 18F-FDG brain positron emission tomography (PET) may reveal reduced metabolism in the frontal and parietal lobes of the cerebrum with normal basal ganglial function, distinguishing ALS from basal ganglial metabolic decline in MSA.
Discussion: To our knowledge, this is the first case of ALS misdiagnosed as MSA. Clinically, patients with parkinsonism who do not respond to dopaminergic drugs should be cautious about atypical ALS. Muscle rigidity manifesting as upper motor neuron damage, and MR and 18F-FDG brain PET imaging can provide early differential diagnosis indicators.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


