Fast Acute Sedation at Intensive Care vs. High-Dose IV Anti-seizure Medication for Treatment of Non-convulsive Status Epilepticus: A Randomized, Multicenter Trial.
Camilla Dyremose Cornwall, Henning Piilgaard, Thorbjørn Søndergaard Engedal, Hanne Tanghus Olsen, Kirsten Møller, Thomas Krøigård, Bülent Uslu, Jakob Christensen, Annette Sidaros, Christoph Patrick Beier
{"title":"Fast Acute Sedation at Intensive Care vs. High-Dose IV Anti-seizure Medication for Treatment of Non-convulsive Status Epilepticus: A Randomized, Multicenter Trial.","authors":"Camilla Dyremose Cornwall, Henning Piilgaard, Thorbjørn Søndergaard Engedal, Hanne Tanghus Olsen, Kirsten Møller, Thomas Krøigård, Bülent Uslu, Jakob Christensen, Annette Sidaros, Christoph Patrick Beier","doi":"10.1097/CCE.0000000000001311","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The management of refractory status epilepticus (SE) remains an area of low evidence with varying management strategies. Treatment in the ICU is often postponed due to potential complications from sedation, and it is unknown if its efficacy is superior to additional treatment attempts with IV anti-seizure medications (ASMs). The Fast Acute Sedation at Intensive Care vs. High-Dose IV Anti-Seizure Medication for Treatment of Non-Convulsive Status Epilepticus (FAST) trial aims to compare the efficacy of rapid sedation in the ICU vs. add-on high-dose IV ASM alone for the treatment of refractory SE.</p><p><strong>Methods/results: </strong>This prospective, randomized, multicenter trial will enroll adult patients with non-convulsive status epilepticus (NCSE) who either meet current EEG criteria or have unambiguous NCSE with minor motor phenomena (\"subtle SE\") but without ongoing tonic-clonic seizures that are refractory to benzodiazepines and treatment with at least one second-line ASM. Patients will be randomized to receive either rapid deep sedation for 20 hours with propofol and eventually low-dose midazolam or additional high-dose IV anticonvulsant therapy (levetiracetam, valproate, fosphenytoin, lacosamide, or topiramate) in the intermediate care unit. The primary endpoint is treatment failure, either defined as NCSE on EEG 24 hours after randomization or persistent NCSE after 3 hours despite therapy on continuous EEG or clinically. Secondary endpoints include assessment of new-onset neurologic deficits and modified Rankin Scale at discharge, economic analyses, length of hospital stay, in-hospital infections, and survival. Evaluations will be performed at baseline, discharge, and 3, 6, 12, and 24 months. The target sample size is 116 patients; we expect to have to randomize about 140 patients to reach the required number of patients.</p><p><strong>Conclusions: </strong>The FAST trial is the first randomized clinical trial to investigate refractory NCSE. Regardless of the outcome, the results of this trial protocol will provide new class 1 evidence for the treatment of NCSE and establish the standard of care for this patient population in the future.</p><p><strong>Trial registration: </strong>EU CT: 2024-515507-18-00/clinicaltrials.gov: NCT05263674.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 9","pages":"e1311"},"PeriodicalIF":2.7000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12440533/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001311","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
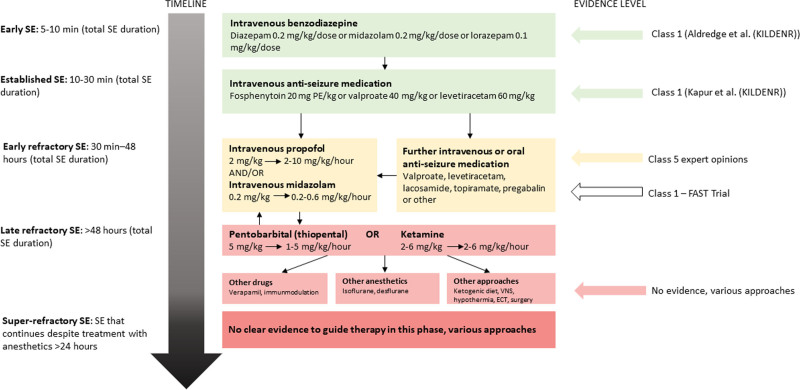
Background: The management of refractory status epilepticus (SE) remains an area of low evidence with varying management strategies. Treatment in the ICU is often postponed due to potential complications from sedation, and it is unknown if its efficacy is superior to additional treatment attempts with IV anti-seizure medications (ASMs). The Fast Acute Sedation at Intensive Care vs. High-Dose IV Anti-Seizure Medication for Treatment of Non-Convulsive Status Epilepticus (FAST) trial aims to compare the efficacy of rapid sedation in the ICU vs. add-on high-dose IV ASM alone for the treatment of refractory SE.
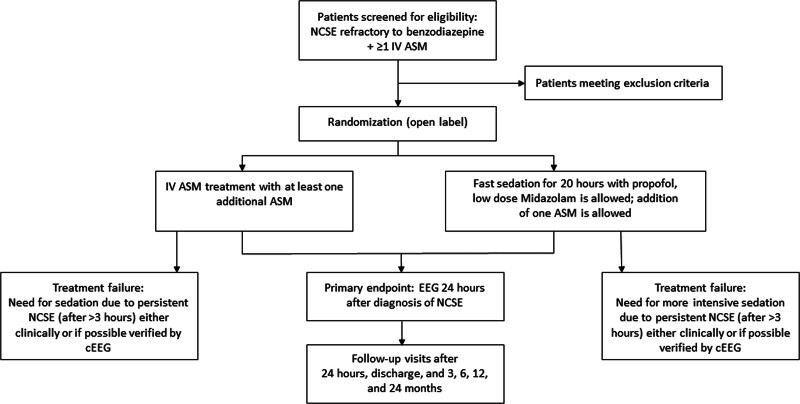
Methods/results: This prospective, randomized, multicenter trial will enroll adult patients with non-convulsive status epilepticus (NCSE) who either meet current EEG criteria or have unambiguous NCSE with minor motor phenomena ("subtle SE") but without ongoing tonic-clonic seizures that are refractory to benzodiazepines and treatment with at least one second-line ASM. Patients will be randomized to receive either rapid deep sedation for 20 hours with propofol and eventually low-dose midazolam or additional high-dose IV anticonvulsant therapy (levetiracetam, valproate, fosphenytoin, lacosamide, or topiramate) in the intermediate care unit. The primary endpoint is treatment failure, either defined as NCSE on EEG 24 hours after randomization or persistent NCSE after 3 hours despite therapy on continuous EEG or clinically. Secondary endpoints include assessment of new-onset neurologic deficits and modified Rankin Scale at discharge, economic analyses, length of hospital stay, in-hospital infections, and survival. Evaluations will be performed at baseline, discharge, and 3, 6, 12, and 24 months. The target sample size is 116 patients; we expect to have to randomize about 140 patients to reach the required number of patients.
Conclusions: The FAST trial is the first randomized clinical trial to investigate refractory NCSE. Regardless of the outcome, the results of this trial protocol will provide new class 1 evidence for the treatment of NCSE and establish the standard of care for this patient population in the future.
Trial registration: EU CT: 2024-515507-18-00/clinicaltrials.gov: NCT05263674.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


