Ye Peng, Xuezhu Qi, Mingzhi Yu, Gongzi Zhang, Moning Guo, Jianpeng Zheng, Lu Feng, Zaihua Wei, Jianting Su, Danhui Yi, Xinyu Liu, Yao Yao, Lihai Zhang
{"title":"Optimizing Surgical Strategies for Elderly Patients With Femoral Neck Fracture: The Critical Role of Comorbidities.","authors":"Ye Peng, Xuezhu Qi, Mingzhi Yu, Gongzi Zhang, Moning Guo, Jianpeng Zheng, Lu Feng, Zaihua Wei, Jianting Su, Danhui Yi, Xinyu Liu, Yao Yao, Lihai Zhang","doi":"10.5435/JAAOSGlobal-D-25-00062","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Femoral neck fractures (FNFs) pose a notable challenge in the elderly population, given the high associated mortality rates and costs. The choice between internal fixation (IF) and hip arthroplasty (HA) has long been debated, yet existing guidelines often overlooked the crucial influence of comorbidities. With the increasing number of hip fracture cases globally and the complexity of patient conditions, it is essential to identify the key factors that truly affect surgical outcomes.</p><p><strong>Methods: </strong>We conducted a large-scale retrospective study across 152 Beijing hospitals, including 25,764 patients aged 60+ years with FNF. After excluding those with severe preexisting conditions, we collected data on patient characteristics and used advanced statistical methods for analysis.</p><p><strong>Results: </strong>Among the patients, 4568 received IF and 21,196 received HA. IF decreased 1-year mortality in patients with fewer than four comorbidities, whereas HA was more beneficial for those with four or more comorbidities. Mortality predicted by comorbidities was notably lower than that by age and sex (2.379% versus 2.790%, P < 0.001), and age had no marked influence on outcomes.</p><p><strong>Conclusion: </strong>In summary, for elderly patients with FNF, comorbidity profile, rather than age or sex, should be the key determinant in surgical choices to reduce all-cause mortality. These findings support the refinement of surgical guidelines and have implications for geriatric care. Future research should focus on enhancing comorbidity assessment in surgical planning.</p>","PeriodicalId":45062,"journal":{"name":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","volume":"9 9","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422777/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5435/JAAOSGlobal-D-25-00062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Femoral neck fractures (FNFs) pose a notable challenge in the elderly population, given the high associated mortality rates and costs. The choice between internal fixation (IF) and hip arthroplasty (HA) has long been debated, yet existing guidelines often overlooked the crucial influence of comorbidities. With the increasing number of hip fracture cases globally and the complexity of patient conditions, it is essential to identify the key factors that truly affect surgical outcomes.
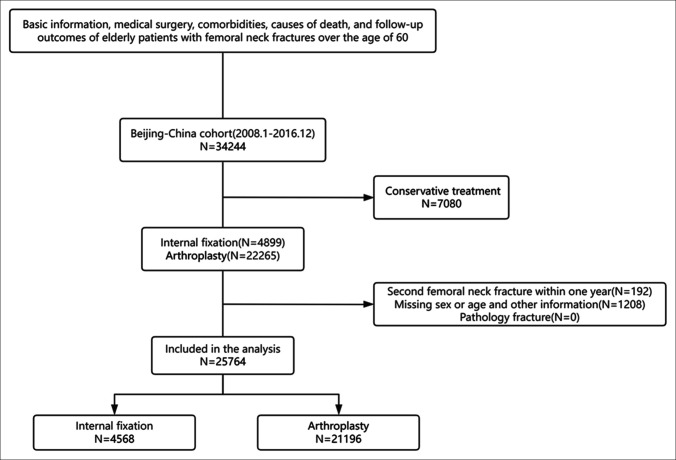
Methods: We conducted a large-scale retrospective study across 152 Beijing hospitals, including 25,764 patients aged 60+ years with FNF. After excluding those with severe preexisting conditions, we collected data on patient characteristics and used advanced statistical methods for analysis.
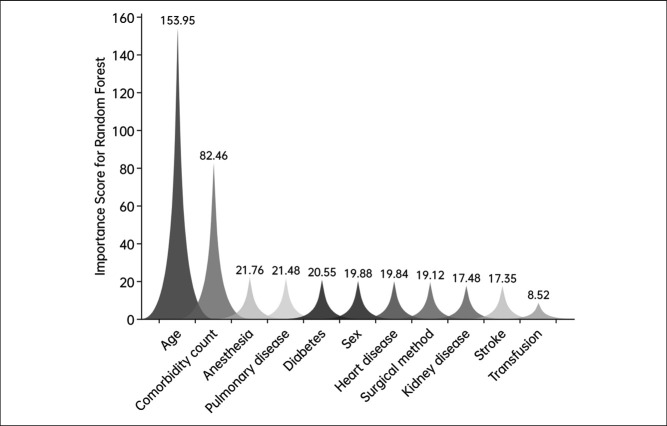
Results: Among the patients, 4568 received IF and 21,196 received HA. IF decreased 1-year mortality in patients with fewer than four comorbidities, whereas HA was more beneficial for those with four or more comorbidities. Mortality predicted by comorbidities was notably lower than that by age and sex (2.379% versus 2.790%, P < 0.001), and age had no marked influence on outcomes.
Conclusion: In summary, for elderly patients with FNF, comorbidity profile, rather than age or sex, should be the key determinant in surgical choices to reduce all-cause mortality. These findings support the refinement of surgical guidelines and have implications for geriatric care. Future research should focus on enhancing comorbidity assessment in surgical planning.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


