Borut Jug, Zlatko Fras, Tjaša Furlan, Marko Novaković, Jerneja Tasič, Mitja Lainščak, Jerneja Farkaš, Dalibor Gavrić, Irena Ograjenšek, Petra Došenović Bonča
{"title":"Uptake and Effectiveness of Outpatient vs. Residential Cardiac Rehabilitation After Myocardial Infarction: A Nationwide Analysis.","authors":"Borut Jug, Zlatko Fras, Tjaša Furlan, Marko Novaković, Jerneja Tasič, Mitja Lainščak, Jerneja Farkaš, Dalibor Gavrić, Irena Ograjenšek, Petra Došenović Bonča","doi":"10.5334/gh.1470","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>To estimate the participation in, and the comparative effectiveness of, short-term residential and comprehensive outpatient cardiac rehabilitation (CR), after the latter was introduced in Slovenia by establishing dedicated regional CR centers.</p><p><strong>Methods: </strong>We extracted and analyzed data on all patients hospitalized for myocardial infarction in Slovenia (<i>n</i> = 15,639), focusing on CR participation - either comprehensive outpatient (introduced in 2017) or short-term residential (available throughout the study period 2015-2021). Impact on nation-wide CR participation rates was assessed by interrupted time series analysis; impact on patient-level outcomes (all-cause mortality and cardiovascular hospitalizations) was assessed using Kaplan Meier estimators and 'doubly robust' Cox regression with propensity score-derived inverse probability of treatment weighting.</p><p><strong>Results: </strong>Of the 11,815 eligible patients (event-free after 180-day landmark), 3819 (32.3%) attended CR. Nation-wide CR participation rates increased both in level (9.7%, 95% CI 6.3-3.1) and in trend (0.41% per month, 95% CI 0.22-0.60) after outpatient CR was introduced in 2017. After propensity score-based adjustment, participation in either CR was associated with lower event rates (12.8%, 17.2%, and 21.0% at 3-year follow-up for outpatient, residential, and no CR, respectively; <i>p</i> < 0.001). Risk reductions were significant for composite outcomes (outpatient: HR 0.58, 95% CI 0.47-0.70; residential: HR 0.79, 95% CI 0.68-0.93) and all-cause mortality (outpatient: HR 0.56, 95% CI 0.38-0.83; residential: HR 0.59, 95% CI 0.45-0.77), whereas the risk reduction for cardiovascular hospitalizations was only significant for outpatient CR (HR 0.60, 95% CI 0.48-0.74). The incremental cost-effectiveness ratio per life-year gained was €6421 and €7381 for outpatient and residential CR, respectively.</p><p><strong>Conclusions: </strong>Participation in either CR improves outcomes after myocardial infarction, but comprehensive outpatient CR conveys superior risk reductions, primarily through reduced cardiovascular hospitalizations.</p><p><strong>Lay summary: </strong>Our study highlights the importance of expanding cardiac rehabilitation services (by setting up dedicated regional comprehensive outpatient centers) and provides new evidence on improved outcomes in patients after myocardial infarction, who undergo cardiac rehabilitation. While previous studies have demonstrated the efficacy and effectiveness of cardiac rehabilitation, ours is the first to compare two distinctive cardiac rehabilitation modalities - comprehensive outpatient (introduced in 2017) and short-term residential (available throughout the study period 2015-2021).In our nationally representative population of patients after myocardial infarction (<i>n</i> = 15,639), participation in cardiac rehabilitation increased both in level (by ~10%) and in trend (by ~0.4% per month) after dedicated cardiac rehabilitation centers were established. Participation in either comprehensive outpatient or short-term residential cardiac rehabilitation was associated with a significant 42% and 21% risk reduction in the primary outcome (death or cardiovascular hospitalization) respectively, after propensity score-based adjustment. Mortality was also reduced (by 46% and 41%, respectively), whereas the risk reduction for hospitalization was only significant in patients undergoing comprehensive cardiac rehabilitation (by 60%).Participation in either cardiac rehabilitation program improves cardiovascular outcomes, but comprehensive outpatient cardiac rehabilitation yields superior risk reductions, primarily through reduced cardiovascular hospitalizations.</p><p><strong>Key learning points: </strong><b>What is already known?:</b> Cardiac rehabilitation improves outcomes in patients with coronary artery disease.Despite its established efficacy, cardiac rehabilitation participation remains suboptimal. Improving access to cardiac rehabilitation through establishing dedicated regional centers may improve participation, but also crowd-out existing options of cardiac rehabilitation.The comparative effectiveness of different cardiac rehabilitation modalities (e.g., comprehensive outpatient versus short-term residential cardiac rehabilitation) remains understudied.<b>What does this study add?:</b> Expanding cardiac rehabilitation services (by setting up dedicated regional comprehensive outpatient centers) significantly improves participation in cardiac rehabilitation after myocardial infarction.Participation in either comprehensive outpatient or short-term residential cardiac rehabilitation after myocardial infarction is associated with improved outcomes (i.e., a significant 42% and 21% risk reduction in death or cardiovascular hospitalization, respectively).Comprehensive outpatient cardiac rehabilitation yields superior risk reductions primarily through reduced cardiovascular hospitalizations.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"80"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12427614/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1470","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
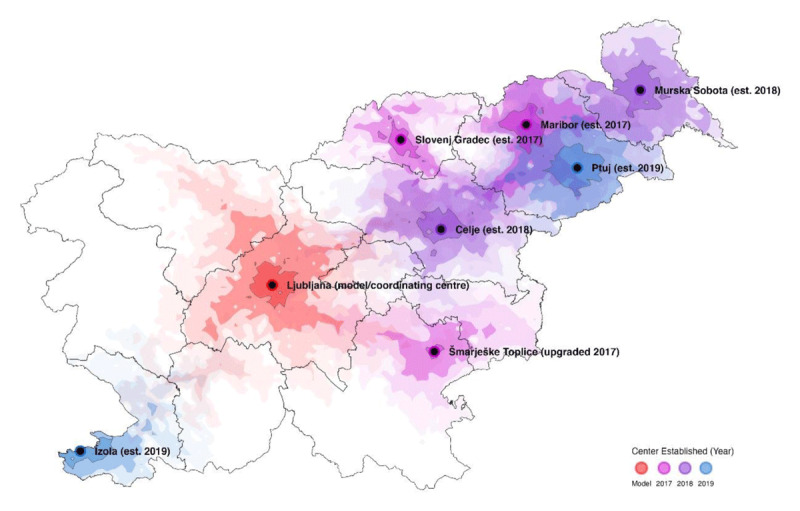
Aims: To estimate the participation in, and the comparative effectiveness of, short-term residential and comprehensive outpatient cardiac rehabilitation (CR), after the latter was introduced in Slovenia by establishing dedicated regional CR centers.
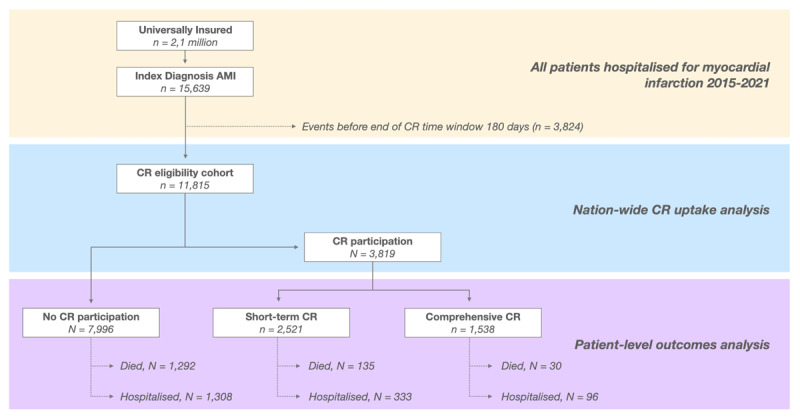
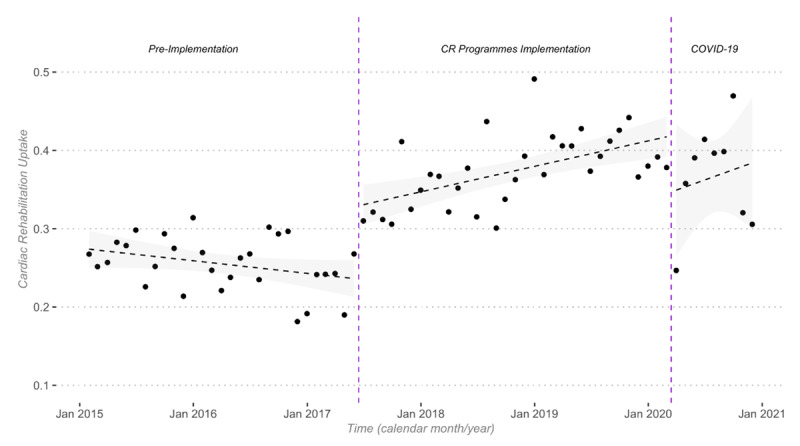
Methods: We extracted and analyzed data on all patients hospitalized for myocardial infarction in Slovenia (n = 15,639), focusing on CR participation - either comprehensive outpatient (introduced in 2017) or short-term residential (available throughout the study period 2015-2021). Impact on nation-wide CR participation rates was assessed by interrupted time series analysis; impact on patient-level outcomes (all-cause mortality and cardiovascular hospitalizations) was assessed using Kaplan Meier estimators and 'doubly robust' Cox regression with propensity score-derived inverse probability of treatment weighting.
Results: Of the 11,815 eligible patients (event-free after 180-day landmark), 3819 (32.3%) attended CR. Nation-wide CR participation rates increased both in level (9.7%, 95% CI 6.3-3.1) and in trend (0.41% per month, 95% CI 0.22-0.60) after outpatient CR was introduced in 2017. After propensity score-based adjustment, participation in either CR was associated with lower event rates (12.8%, 17.2%, and 21.0% at 3-year follow-up for outpatient, residential, and no CR, respectively; p < 0.001). Risk reductions were significant for composite outcomes (outpatient: HR 0.58, 95% CI 0.47-0.70; residential: HR 0.79, 95% CI 0.68-0.93) and all-cause mortality (outpatient: HR 0.56, 95% CI 0.38-0.83; residential: HR 0.59, 95% CI 0.45-0.77), whereas the risk reduction for cardiovascular hospitalizations was only significant for outpatient CR (HR 0.60, 95% CI 0.48-0.74). The incremental cost-effectiveness ratio per life-year gained was €6421 and €7381 for outpatient and residential CR, respectively.
Conclusions: Participation in either CR improves outcomes after myocardial infarction, but comprehensive outpatient CR conveys superior risk reductions, primarily through reduced cardiovascular hospitalizations.
Lay summary: Our study highlights the importance of expanding cardiac rehabilitation services (by setting up dedicated regional comprehensive outpatient centers) and provides new evidence on improved outcomes in patients after myocardial infarction, who undergo cardiac rehabilitation. While previous studies have demonstrated the efficacy and effectiveness of cardiac rehabilitation, ours is the first to compare two distinctive cardiac rehabilitation modalities - comprehensive outpatient (introduced in 2017) and short-term residential (available throughout the study period 2015-2021).In our nationally representative population of patients after myocardial infarction (n = 15,639), participation in cardiac rehabilitation increased both in level (by ~10%) and in trend (by ~0.4% per month) after dedicated cardiac rehabilitation centers were established. Participation in either comprehensive outpatient or short-term residential cardiac rehabilitation was associated with a significant 42% and 21% risk reduction in the primary outcome (death or cardiovascular hospitalization) respectively, after propensity score-based adjustment. Mortality was also reduced (by 46% and 41%, respectively), whereas the risk reduction for hospitalization was only significant in patients undergoing comprehensive cardiac rehabilitation (by 60%).Participation in either cardiac rehabilitation program improves cardiovascular outcomes, but comprehensive outpatient cardiac rehabilitation yields superior risk reductions, primarily through reduced cardiovascular hospitalizations.
Key learning points: What is already known?: Cardiac rehabilitation improves outcomes in patients with coronary artery disease.Despite its established efficacy, cardiac rehabilitation participation remains suboptimal. Improving access to cardiac rehabilitation through establishing dedicated regional centers may improve participation, but also crowd-out existing options of cardiac rehabilitation.The comparative effectiveness of different cardiac rehabilitation modalities (e.g., comprehensive outpatient versus short-term residential cardiac rehabilitation) remains understudied.What does this study add?: Expanding cardiac rehabilitation services (by setting up dedicated regional comprehensive outpatient centers) significantly improves participation in cardiac rehabilitation after myocardial infarction.Participation in either comprehensive outpatient or short-term residential cardiac rehabilitation after myocardial infarction is associated with improved outcomes (i.e., a significant 42% and 21% risk reduction in death or cardiovascular hospitalization, respectively).Comprehensive outpatient cardiac rehabilitation yields superior risk reductions primarily through reduced cardiovascular hospitalizations.
目的:通过建立专门的区域心脏康复中心,估计短期住院和综合门诊心脏康复(CR)在斯洛文尼亚引入后的参与情况和相对有效性。方法:我们提取并分析了斯洛文尼亚因心肌梗死住院的所有患者的数据(n = 15,639),重点关注CR参与-无论是综合门诊(2017年引入)还是短期住院(在2015-2021年期间提供)。通过中断时间序列分析评估对全国CR参与率的影响;对患者水平结果(全因死亡率和心血管住院率)的影响使用Kaplan Meier估计器和“双稳健”Cox回归与倾向评分衍生的治疗加权逆概率进行评估。结果:在11,815例符合条件的患者(180天里程碑后无事件)中,3819例(32.3%)参加了CR。2017年引入门诊CR后,全国CR参与率在水平(9.7%,95% CI 6.3-3.1)和趋势(每月0.41%,95% CI 0.22-0.60)上均有所增加。在基于倾向评分的调整后,参与任何CR均与较低的事件发生率相关(门诊、住院和无CR的3年随访分别为12.8%、17.2%和21.0%;p < 0.001)。综合结果(门诊:HR 0.58, 95% CI 0.47-0.70;住院:HR 0.79, 95% CI 0.68-0.93)和全因死亡率(门诊:HR 0.56, 95% CI 0.38-0.83;住院:HR 0.59, 95% CI 0.45-0.77)的风险降低显著,而心血管住院的风险降低仅在门诊CR (HR 0.60, 95% CI 0.48-0.74)中显著。门诊和住院CR的增量成本效益比分别为6421欧元和7381欧元。结论:参与两种CR均可改善心肌梗死后的预后,但综合门诊CR可显著降低风险,主要是通过减少心血管住院。摘要:我们的研究强调了扩大心脏康复服务的重要性(通过建立专门的区域综合门诊中心),并为心肌梗死后接受心脏康复治疗的患者改善预后提供了新的证据。虽然之前的研究已经证明了心脏康复的疗效和有效性,但我们的研究首次比较了两种不同的心脏康复模式——综合门诊(2017年引入)和短期住院(2015-2021年期间提供)。在我们具有全国代表性的心肌梗死患者人群中(n = 15,639),在专门的心脏康复中心建立后,心脏康复的参与水平(约10%)和趋势(每月约0.4%)都有所增加。在基于倾向评分的调整后,参加综合门诊或短期住院心脏康复与主要结局(死亡或心血管住院)分别显著降低42%和21%的风险相关。死亡率也降低(分别为46%和41%),而住院风险降低仅在接受全面心脏康复的患者中显著(降低60%)。参与任何一项心脏康复计划都能改善心血管预后,但综合门诊心脏康复主要通过减少心血管住院治疗,可显著降低风险。学习要点:什么是已知的?心脏康复可改善冠心病患者的预后。尽管其已确立的疗效,心脏康复参与仍然是次优的。通过建立专门的区域中心来改善心脏康复的可及性可能会提高参与度,但也会挤占现有的心脏康复选择。不同心脏康复方式(例如,综合门诊与短期住院心脏康复)的比较效果仍未得到充分研究。这项研究补充了什么?扩大心脏康复服务(设立专门的区域综合门诊中心),显著提高心肌梗死后心脏康复的参与率。心肌梗死后参加综合门诊或短期住院心脏康复与改善预后相关(即,死亡或心血管住院的风险分别显著降低42%和21%)。综合门诊心脏康复主要通过减少心血管住院产生优越的风险降低。
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


