Summary of best evidence for enhanced recovery after surgery for perioperative management of pediatric cleft lip and palate surgery: a narrative review.
{"title":"Summary of best evidence for enhanced recovery after surgery for perioperative management of pediatric cleft lip and palate surgery: a narrative review.","authors":"Chenxin Zhang, Junyi Guo, Sijia Chen, Yuying Zhou, Lingxuan Zhu","doi":"10.21037/tp-2025-318","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Children with cleft lip and palate face more complex stressful situations in the perioperative period due to their underdeveloped systems and relatively weaker resistance to various injurious stimuli. The concept of enhanced recovery after surgery (ERAS) offers a novel perspective on the perioperative management of pediatric patients with cleft lip and palate. This narrative review aimed to search, evaluate, and summarize the best evidence for ERAS in children with cleft lip and palate, and provide reference for clinical perioperative nursing practice.</p><p><strong>Methods: </strong>We searched the databases of The British Medical Journal (BMJ), UpToDate, The Cochrane Library, Guidelines International Network (GIN), Scottish Intercollegiate Guidelines Network (SIGN), Joanna Briggs Institute (JBI), Medlive, American Cleft Palate-Craniofacial Association (ACPA), Enhanced Recovery After Surgery Society, Chinese Stomatological Association (CSA), PubMed, Web of Science, Embase, Scopus, SinoMed, China National Knowledge Infrastructure (CNKI), Wanfang, and China Science and Technology Journal (VIP). The search covered the period from the database's inception to December 2024. This study included children undergoing congenital cleft lip and palate surgery who received perioperative ERAS interventions with evidence derived from guidelines, evidence summary, expert consensus, systematic reviews, or randomized controlled trials (RCTs), while excluding non-English/Chinese literature, incomplete methodological details or low-quality appraisal ratings, and studies with unavailable data. Quality was assessed using Clinical Guidelines Research and Evaluation System for guidelines, Critical Appraisal for Summaries of Evidence for evidence summaries, the JBI Critical Appraisal Tool for Systematic Reviews, the JBI Critical Appraisal Checklists for expert consensus, and the Cochrane Risk of Bias Tool for randomized trials. Evidence synthesis was performed using the JBI Evidence Pre-grading System (2014) to classify evidence levels (1-5), followed by recommendation grading (grade A/B).</p><p><strong>Key content and findings: </strong>A total of 14 articles were included, including four guidelines, one technical report, two expert consensus articles, three systematic reviews, and four RCTs (covering 342 patients). The publication or update dates of these studies spanned 2019-2024, with their sources predominantly originating from the United States and China, and they covered the entire perioperative period. Through a comprehensive analysis of these studies, 17 themes and 34 recommendations were identified in total. These recommendations cover preoperative preparation (health education, nutrition, fasting), intraoperative care (anesthesia, temperature), postoperative management (pain, feeding, wound care), and discharge follow-up.</p><p><strong>Conclusions: </strong>This study synthesizes 34 key evidence-based recommendations for perioperative ERAS management in pediatric cleft lip and palate surgery, providing structured guidance to accelerate postoperative recovery and standardize clinical practice. Since these findings originated from several nations, institution-specific factors must be assessed prior to adoption of ERAS protocols. These factors include resource availability, local healthcare policies, multidisciplinary team engagement, and existing clinical workflows.</p>","PeriodicalId":23294,"journal":{"name":"Translational pediatrics","volume":"14 8","pages":"2009-2022"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433080/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tp-2025-318","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: Children with cleft lip and palate face more complex stressful situations in the perioperative period due to their underdeveloped systems and relatively weaker resistance to various injurious stimuli. The concept of enhanced recovery after surgery (ERAS) offers a novel perspective on the perioperative management of pediatric patients with cleft lip and palate. This narrative review aimed to search, evaluate, and summarize the best evidence for ERAS in children with cleft lip and palate, and provide reference for clinical perioperative nursing practice.
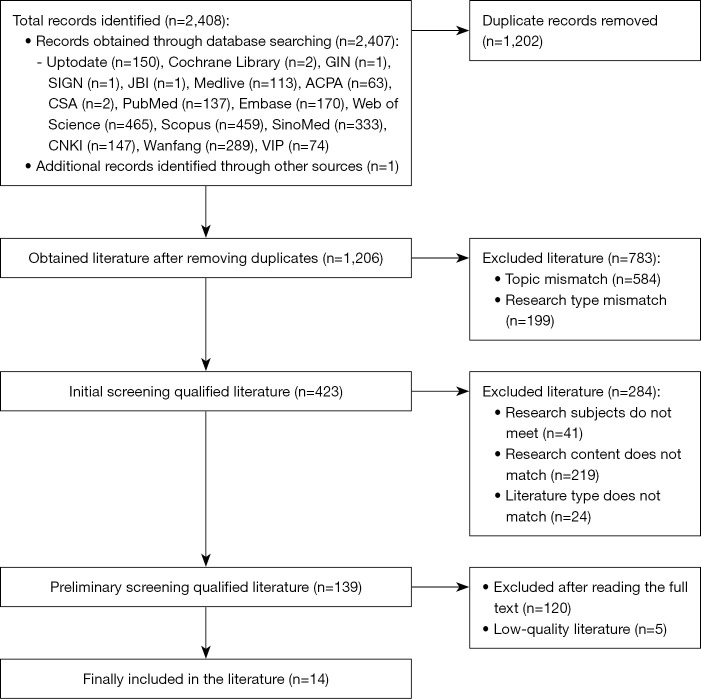
Methods: We searched the databases of The British Medical Journal (BMJ), UpToDate, The Cochrane Library, Guidelines International Network (GIN), Scottish Intercollegiate Guidelines Network (SIGN), Joanna Briggs Institute (JBI), Medlive, American Cleft Palate-Craniofacial Association (ACPA), Enhanced Recovery After Surgery Society, Chinese Stomatological Association (CSA), PubMed, Web of Science, Embase, Scopus, SinoMed, China National Knowledge Infrastructure (CNKI), Wanfang, and China Science and Technology Journal (VIP). The search covered the period from the database's inception to December 2024. This study included children undergoing congenital cleft lip and palate surgery who received perioperative ERAS interventions with evidence derived from guidelines, evidence summary, expert consensus, systematic reviews, or randomized controlled trials (RCTs), while excluding non-English/Chinese literature, incomplete methodological details or low-quality appraisal ratings, and studies with unavailable data. Quality was assessed using Clinical Guidelines Research and Evaluation System for guidelines, Critical Appraisal for Summaries of Evidence for evidence summaries, the JBI Critical Appraisal Tool for Systematic Reviews, the JBI Critical Appraisal Checklists for expert consensus, and the Cochrane Risk of Bias Tool for randomized trials. Evidence synthesis was performed using the JBI Evidence Pre-grading System (2014) to classify evidence levels (1-5), followed by recommendation grading (grade A/B).
Key content and findings: A total of 14 articles were included, including four guidelines, one technical report, two expert consensus articles, three systematic reviews, and four RCTs (covering 342 patients). The publication or update dates of these studies spanned 2019-2024, with their sources predominantly originating from the United States and China, and they covered the entire perioperative period. Through a comprehensive analysis of these studies, 17 themes and 34 recommendations were identified in total. These recommendations cover preoperative preparation (health education, nutrition, fasting), intraoperative care (anesthesia, temperature), postoperative management (pain, feeding, wound care), and discharge follow-up.
Conclusions: This study synthesizes 34 key evidence-based recommendations for perioperative ERAS management in pediatric cleft lip and palate surgery, providing structured guidance to accelerate postoperative recovery and standardize clinical practice. Since these findings originated from several nations, institution-specific factors must be assessed prior to adoption of ERAS protocols. These factors include resource availability, local healthcare policies, multidisciplinary team engagement, and existing clinical workflows.
背景与目的:唇腭裂患儿由于系统发育不完善,对各种有害刺激的抵抗力相对较弱,围手术期面临较为复杂的应激情境。术后增强恢复(ERAS)的概念为唇腭裂患儿的围手术期治疗提供了一个新的视角。本文旨在寻找、评价和总结唇腭裂患儿ERAS的最佳证据,为临床围手术期护理提供参考。方法:我们检索了英国医学杂志(BMJ)、UpToDate、Cochrane图书馆、指南国际网络(GIN)、苏格兰校际指南网络(SIGN)、Joanna Briggs研究所(JBI)、Medlive、美国腭裂颅面协会(ACPA)、术后增强康复学会、中国口腔医学会(CSA)、PubMed、Web of Science、Embase、Scopus、中国医学信息中心(sinmed)、中国知网(CNKI)、万方、《中国科技学报》(VIP)。搜索涵盖了从数据库建立到2024年12月的这段时间。本研究纳入了接受先天性唇腭裂手术围手术期ERAS干预的患儿,其证据来自指南、证据总结、专家共识、系统评价或随机对照试验(rct),同时排除了非中英文文献、方法学细节不完整或低质量评价评分以及数据不可用的研究。质量评估采用临床指南研究与评价系统(临床指南研究与评价系统)、证据摘要关键评价系统(证据摘要关键评价系统)、JBI系统评价关键评价工具(专家共识关键评价清单)和Cochrane随机试验偏倚风险工具(随机试验)。使用JBI证据预分级系统(2014)进行证据综合,对证据等级(1-5)进行分类,然后进行建议分级(A/B级)。主要内容和发现:共纳入14篇文章,包括4篇指南、1篇技术报告、2篇专家共识文章、3篇系统评价和4篇随机对照试验(涵盖342例患者)。这些研究的发表或更新日期跨越2019-2024年,其来源主要来自美国和中国,涵盖了整个围手术期。通过对这些研究的综合分析,共确定了17个主题和34项建议。这些建议包括术前准备(健康教育、营养、禁食)、术中护理(麻醉、温度)、术后管理(疼痛、喂养、伤口护理)和出院随访。结论:本研究综合了34项关键循证建议,为儿童唇腭裂手术围手术期ERAS管理提供结构化指导,加快术后恢复,规范临床实践。由于这些调查结果来自几个国家,因此必须在采用ERAS协议之前评估机构特定因素。这些因素包括资源可用性、当地医疗保健政策、多学科团队参与和现有临床工作流程。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


