{"title":"Arthritis associated with Kawasaki disease after initial combination therapy with cyclosporine: a case report.","authors":"Kaori Yoshida, Yoshitaka Watanabe, Maria Yoshimi, Nobuhiro Kawai, Minako Matsumoto, Hirokazu Ikeda","doi":"10.21037/tp-2025-176","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Since the 2020 revision of the Kawasaki disease (KD) treatment guidelines, there have been few reports of reactive arthritis secondary to treatment-resistant KD. This study reports a case of KD that required initial treatment with cyclosporine A (CyA) followed by additional infliximab (IFX) and secondary to reactive arthritis.</p><p><strong>Case description: </strong>A 5-year-old boy met diagnostic criteria for KD on day 5 of fever and had an intravenous immunoglobulin (IVIG) refractory predictive score of 8 (≥5) was administered ulinastatin, IFX, and three IVIG doses in combination with CyA. His fever resolved on day 9. Subsequently, acetylsalicylic acid was changed to flurbiprofen and then to dipyridamole due to suspicion of a drug rash. Fever and pain appeared in ankle joints and right hip joint on day 18 of illness. Prednisolone (PSL) was started on day 23 of illness for reactive arthritis associated with KD, which improved the joint pain. No recurrence of joint symptoms or coronary artery lesions was observed after tapering off of PSL.</p><p><strong>Conclusions: </strong>Based on the evaluation at the start of treatment, although CyA is initially administered in potential IVIG-resistant patients, attention must be paid to secondary reactive arthritis if the patient becomes resistant to treatment and requires IFX treatment.</p>","PeriodicalId":23294,"journal":{"name":"Translational pediatrics","volume":"14 8","pages":"2042-2046"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433033/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tp-2025-176","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Since the 2020 revision of the Kawasaki disease (KD) treatment guidelines, there have been few reports of reactive arthritis secondary to treatment-resistant KD. This study reports a case of KD that required initial treatment with cyclosporine A (CyA) followed by additional infliximab (IFX) and secondary to reactive arthritis.
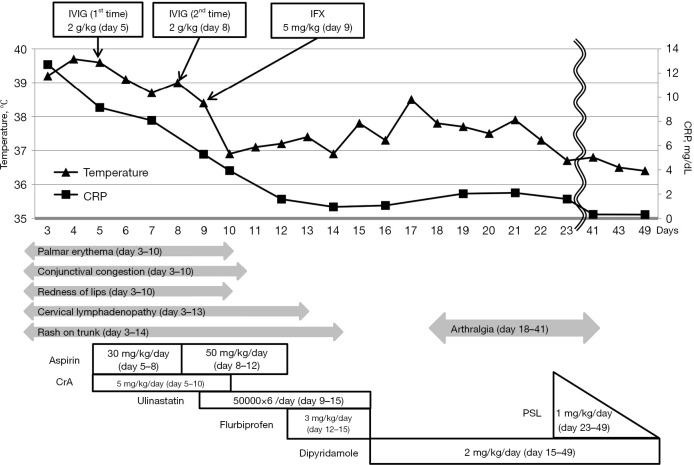
Case description: A 5-year-old boy met diagnostic criteria for KD on day 5 of fever and had an intravenous immunoglobulin (IVIG) refractory predictive score of 8 (≥5) was administered ulinastatin, IFX, and three IVIG doses in combination with CyA. His fever resolved on day 9. Subsequently, acetylsalicylic acid was changed to flurbiprofen and then to dipyridamole due to suspicion of a drug rash. Fever and pain appeared in ankle joints and right hip joint on day 18 of illness. Prednisolone (PSL) was started on day 23 of illness for reactive arthritis associated with KD, which improved the joint pain. No recurrence of joint symptoms or coronary artery lesions was observed after tapering off of PSL.
Conclusions: Based on the evaluation at the start of treatment, although CyA is initially administered in potential IVIG-resistant patients, attention must be paid to secondary reactive arthritis if the patient becomes resistant to treatment and requires IFX treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


