Influential factors affecting the survival benefit of combined neoadjuvant therapy and esophagectomy in patients with esophageal cancer: an analysis based on the SEER database.
{"title":"Influential factors affecting the survival benefit of combined neoadjuvant therapy and esophagectomy in patients with esophageal cancer: an analysis based on the SEER database.","authors":"Mi Chen, Li Jia, Zhou Su","doi":"10.21037/tcr-2025-543","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Esophageal cancer (EC) is a major contributor to cancer-related deaths globally, with significant mortality rates. Neoadjuvant therapy (NAT), involving preoperative chemotherapy or radiation, aims to enhance outcomes in EC when combined with esophagectomy. However, its efficacy varies, necessitating identification of factors influencing survival benefits. This study aims to identify the factors influencing the survival benefit of NAT in patients with EC.</p><p><strong>Methods: </strong>The current retrospective cohort study collected data from the Surveillance, Epidemiology and End Results (SEER) database between 2004 and 2015. Propensity score matching (PSM) was used to balance baseline characteristics between the NAT and No NAT groups. A Cox model-based residual approach was applied to estimate the likelihood of survival benefit. Logistic regression was used to explore associated factors in the training cohort, and a nomogram was subsequently developed and validated.</p><p><strong>Results: </strong>In total, 2,755 patients were included in this study. Before PSM, the NAT group had a significantly longer median overall survival (mOS) than the No NAT group (31 <i>vs.</i> 21 months, P<0.001). After PSM, the survival advantage of the NAT group persisted (24 <i>vs.</i> 21 months, P=0.03). In the training cohort, tumor (T) stage, metastasis (M) stage, tumor grade, and lymph node ratio (LNR) appeared to be associated with survival benefit among patients receiving NAT. A nomogram was subsequently constructed based on these factors to estimate the likelihood of deriving benefit from NAT. In the validation cohort, the model exhibited reasonable discriminatory performance, with an area under the receiver operating characteristic (ROC) curve (AUC) of 0.782.</p><p><strong>Conclusions: </strong>This study identified clinical features potentially associated with survival benefit from NAT in patients with EC. The nomogram may serve as a reference tool to support treatment planning and patient selection in clinical practice.</p>","PeriodicalId":23216,"journal":{"name":"Translational cancer research","volume":"14 8","pages":"4837-4850"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432777/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational cancer research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tcr-2025-543","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/26 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Esophageal cancer (EC) is a major contributor to cancer-related deaths globally, with significant mortality rates. Neoadjuvant therapy (NAT), involving preoperative chemotherapy or radiation, aims to enhance outcomes in EC when combined with esophagectomy. However, its efficacy varies, necessitating identification of factors influencing survival benefits. This study aims to identify the factors influencing the survival benefit of NAT in patients with EC.
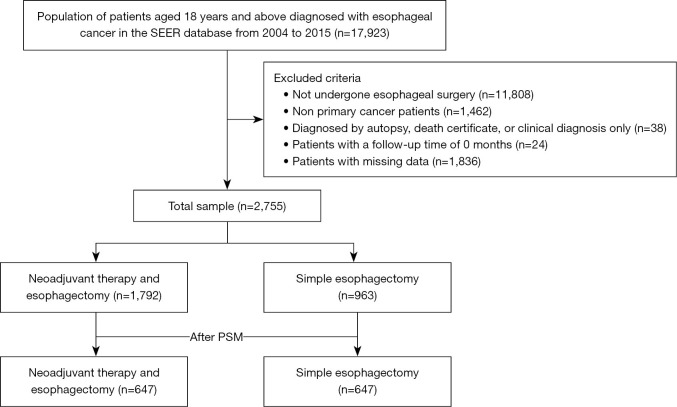
Methods: The current retrospective cohort study collected data from the Surveillance, Epidemiology and End Results (SEER) database between 2004 and 2015. Propensity score matching (PSM) was used to balance baseline characteristics between the NAT and No NAT groups. A Cox model-based residual approach was applied to estimate the likelihood of survival benefit. Logistic regression was used to explore associated factors in the training cohort, and a nomogram was subsequently developed and validated.
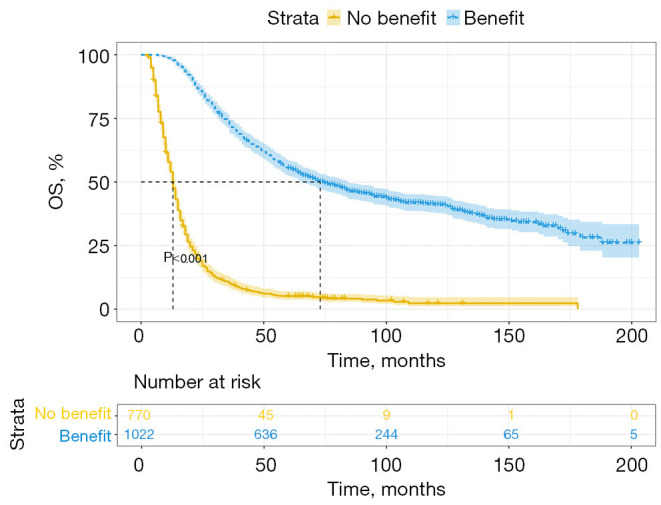
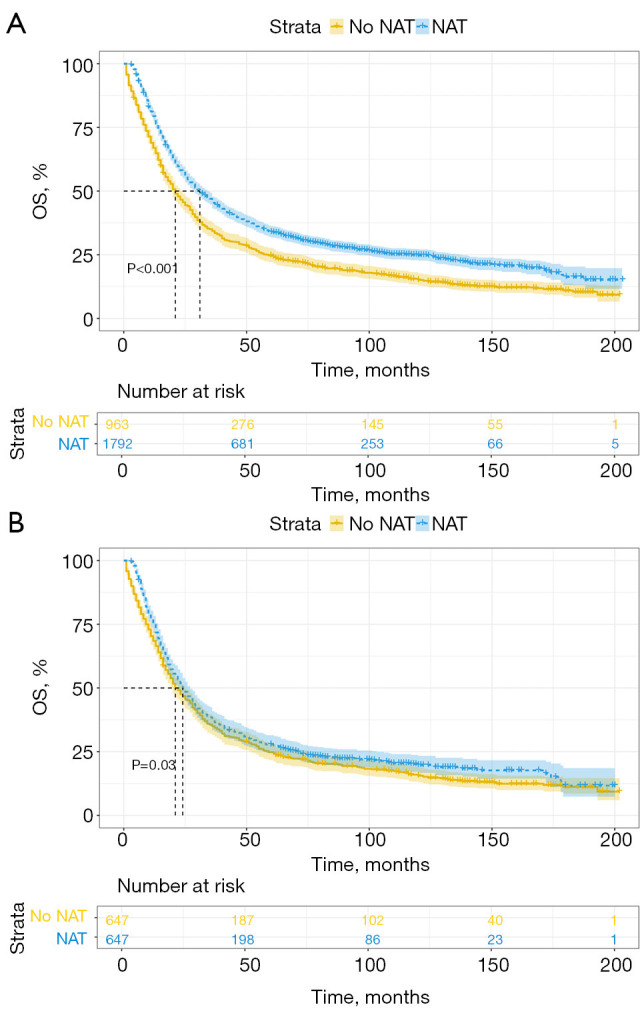
Results: In total, 2,755 patients were included in this study. Before PSM, the NAT group had a significantly longer median overall survival (mOS) than the No NAT group (31 vs. 21 months, P<0.001). After PSM, the survival advantage of the NAT group persisted (24 vs. 21 months, P=0.03). In the training cohort, tumor (T) stage, metastasis (M) stage, tumor grade, and lymph node ratio (LNR) appeared to be associated with survival benefit among patients receiving NAT. A nomogram was subsequently constructed based on these factors to estimate the likelihood of deriving benefit from NAT. In the validation cohort, the model exhibited reasonable discriminatory performance, with an area under the receiver operating characteristic (ROC) curve (AUC) of 0.782.
Conclusions: This study identified clinical features potentially associated with survival benefit from NAT in patients with EC. The nomogram may serve as a reference tool to support treatment planning and patient selection in clinical practice.
期刊介绍:
Translational Cancer Research (Transl Cancer Res TCR; Print ISSN: 2218-676X; Online ISSN 2219-6803; http://tcr.amegroups.com/) is an Open Access, peer-reviewed journal, indexed in Science Citation Index Expanded (SCIE). TCR publishes laboratory studies of novel therapeutic interventions as well as clinical trials which evaluate new treatment paradigms for cancer; results of novel research investigations which bridge the laboratory and clinical settings including risk assessment, cellular and molecular characterization, prevention, detection, diagnosis and treatment of human cancers with the overall goal of improving the clinical care of cancer patients. The focus of TCR is original, peer-reviewed, science-based research that successfully advances clinical medicine toward the goal of improving patients'' quality of life. The editors and an international advisory group of scientists and clinician-scientists as well as other experts will hold TCR articles to the high-quality standards. We accept Original Articles as well as Review Articles, Editorials and Brief Articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


